
1-Adénomyose-Echo
Présence de kystes anéchogènes (►) de taille variée, et hyperéchogènes hématiques (►), situés dans le myomètre, à proximité de l’interface endomètre- myomètre : adénomyose interne.
Endomètre (★).
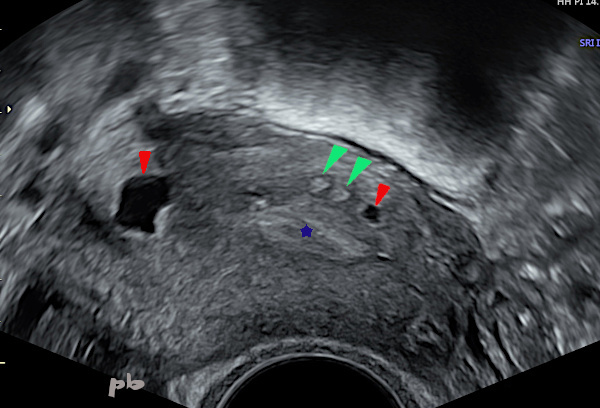
1-Adenomyosis-Ultrasound
Presence of anechoic cysts (►) of varying sizes, and hyperechoic hemorrhagic cysts (►), located in the myometrium, near the endometrium-myometrium interface : internal adenomyosis.
Endometrium (★).

2-Adénomyose-Echo doppler
Multiples images hyperéchogènes ( ► ) donnant à l’interface endomètre-myomètre un aspect irrégulier. Elles correspondent à la présence de glandes endométriales dans le myomètre.
Endomètre (★). La ligne cavitaire est bien visible.
Une plage hyperéchogène plus importante, sans flux en doppler couleur (★) : kyste hématique probable.
2-Adenomyosis – Doppler Ultrasound
Multiple hyperechoic images (►) giving the endometrium-myometrium interface an irregular appearance. They correspond to the presence of endometrial glands in the myometrium.
Endometrium (★). The cavity line is clearly visible.
A larger hyperechoic area, without flow on color Doppler (★): probable hemorrhagic cyst.

3-Adénomyose interne – Echo
Présence de plusieurs images hyperéchogènes (►) sous-endométriales arrondies.
L’endomètre reste bien visible malgré tout.
3-Internal Adenomyosis – Ultrasound
Presence of several rounded sub-endometrial hyperechoic images (►).
The endometrium remains clearly visible nonetheless.

4-Adénomyose – Hystérographie (HSG)
(même patiente que 3)
Images d’addition au niveau de la corne utérine gauche : opacification des glandes endométriales situées dans le myomètre. Ce sont les 1ères images historiquement connues de l’adénomyose en radiologie. Mais l’adénomyose n’est plus depuis longtemps une indication à l’HSG (il s’agit d’un dossier de 1997).
Ces images de « flammèches » ou « boule de gui » correspondent aux images hyperéchogènes échographiques.
Cavité utérine ( ★ )
Segment interstitiel puis isthmique de la trompe gauche ( ►)
4-Adenomyosis – Hysterosalpingography (same patient as 3)
Images of addition at the level of the left uterine horn : opacification of the endometrial glands located in the myometrium. These are the first historically known images of adenomyosis in radiology. However, adenomyosis has not been an indication for HSG for a long time (this is a case from 1997).
These images of multiple small outpouchings of the contrast material correspond to the hyperechoic ultrasound images.
Uterine cavity (★)
Interstitial and then isthmic segment of the left tube (►)
5 – Adénomyose interne – Echo
Coupe frontale 2D de la cavité utérine par voie vaginale (utérus latéro-dévié).
L’interface endomètre-myomètre est parfaitement régulière en latéral (♦︎), alors qu’elle apparait très irrégulière et floue au niveau fundique (étoiles blanches).
Kystes anéchogènes (►) et images hyperéchogènes sous-endométriales fundiques (►).
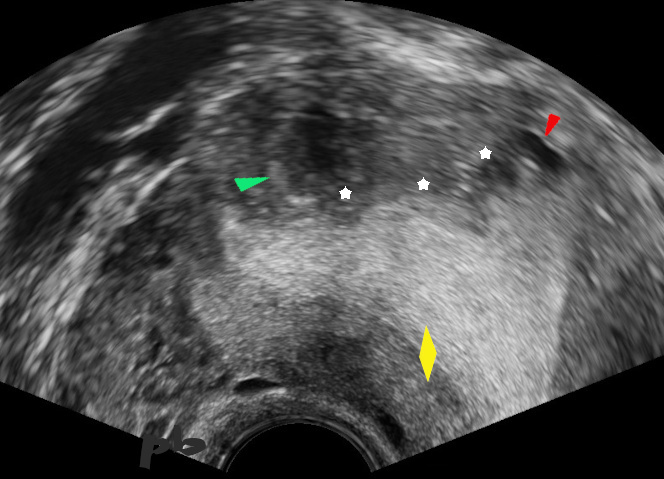
5 – Internal Adenomyosis – Ultrasound
2D frontal section of the uterine cavity via vaginal route (laterally deviated uterus).
The endometrium-myometrium interface is perfectly regular laterally (♦), whereas it appears very irregular and blurred at the fundal level (white stars).
Anechoic cysts (►) and hyperechoic sub-endometrial fundal images (►).

6-Adénomyose interne – IRM
Coupe axiale T2 réalisant une coupe frontale de l’utérus (« hystérographique »).
Même aspect en IRM de « flammèche » (►), située au sein d’une zone jonctionnelle en hyposignal T2 élargie (►)
La corne droite adjacente présente un aspect érigé, image décrite depuis longtemps en HSG.
6-Internal Adenomyosis – MRI
Axial T2 section creating a frontal section of the uterus (‘hysterosalpingographic’).
Same MRI appearance of ‘sparks’ (►), located within an enlarged junctional zone in T2 hypointensity (►).
The adjacent right horn has an erect appearance, an image that has long been described in HSG.
7-Adénomyose diffuse – écho voie sus-pubienne
Coupe sagittale : volumineux utérus, comme le montre ses mensurations en bas de l’image, non déformé.
Le myomètre présente un aspect hétérogène, « mité », sans image focale individualisable.
L’endomètre ( ► ) reste centré, mais est difficile à délimiter.
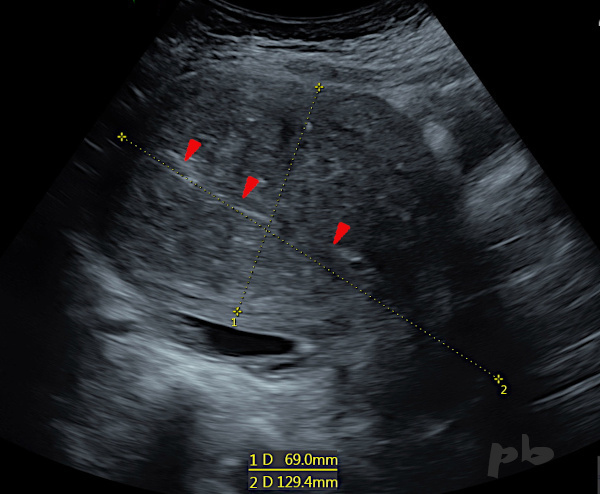
7-Diffuse Adenomyosis – Transabdominal Ultrasound
Sagittal section : large uterus, as shown by its measurements at the bottom of the image, not deformed.
The myometrium has a heterogeneous, ‘moth-eaten’, Swiss cheese appearance, without any identifiable focal image.
The endometrium (►) remains centered but is difficult to delineate.
8-Adénomyose diffuse– Echo endovaginale (même patiente que 7)
Gros utérus.
Myomètre hétérogène et atténuant, d’échogénicité augmentée. De ce fait, l’endomètre n’est pas visible. La lumière utérine n’apparait qu’au niveau cervico-isthmique (►).
Fond utérin (♦︎).
(Un exemple de l’intérêt à pratiquer systématiquement une voie sus-pubienne).
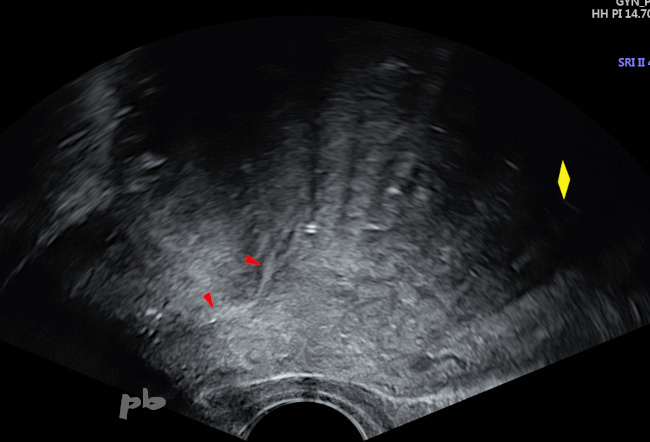
8-Diffuse Adenomyosis – Transvaginal Ultrasound (same patient as 7)
Large uterus. Heterogeneous and attenuating myometrium with increased echogenicity. As a result, the endometrium is not visible. The uterine cavity is only apparent at the cervico-isthmic level (►).
Uterine fundus (♦︎).
(An example of the importance of systematically performing a suprapubic approach).

9-Adénomyose diffuse – IRM (même patiente que 7)
Sagittal T2.
Volumineux utérus, remontant au-delà du promontoire. Myomètre globalement hyposignal, zone jonctionnelle prédominante (ZJ).
L’endomètre est cette fois bien visible (►), parfaitement fin et régulier.
Nombreux petits kystes myométriaux en hypersignal (►).
L’IRM est particulièrement utile dans un contexte de métrorragie lorsque l’endomètre est mal analysé en échographie.
9-Diffuse Adenomyosis – MRI (same patient as 7)
Sagittal T2 section.
Large uterus, extending beyond the promontory. Hypointense myometrium with a predominant junctional zone (JZ).
The endometrium is clearly visible this time (►), perfectly thin and regular.
Numerous small myometrial cysts in hyperintense signal (►).
MRI is particularly useful in the context of metrorrhagia when the endometrium is poorly analyzed by ultrasound.

10-Adénomyose diffuse – IRM (même patiente que 7)
Axial T1
2 petits kystes hématiques en hyper T1 ( ► ).
Par ailleurs, hématosalpinx ( ★ ) en rétro-utérin.
10-Diffuse Adenomyosis – MRI (same patient as 7)
Axial T1
Two small hemorrhagic cysts in hyper T1 (►).
Additionally, hemosalpinx (★) in the retro-uterine area.

11- Adénomyose diffuse – Hystérographie (HSG)
Même patiente que 7
HSG réalisée dans le cadre d’un bilan d’infertilité.
On retrouve les signes classiques de l’adénomyose :
-l’aspect de cornes utérines « érigées » (►)
-Les nombreuses images d’addition au niveau du fond utérin ( ► ), en « flammèches ».
L’infertilité s’explique surtout par l’obstruction tubaire bilatérale (★) et non par l’adénomyose (hématosalpinx sur l’IRM : image 10) .
11-Diffuse Adenomyosis – Hysterosalpingography (HSG)
Same patient as 7
HSG performed as part of an infertility assessment.
We find the classic signs of adenomyosis :
-the appearance of ‘erected’ uterine horns (►)
-the numerous additional images at the uterine fundus (►), in a ‘flame-like’ pattern.
The infertility is mainly explained by bilateral tubal obstruction (★) and not by adenomyosis (hematosalpinx on MRI : image 10)
© Dr Philippe BASSNAGEL – 2021