

1 – Pseudo-vessie
Echographie voie sus-pubienne.
L’aspect échographique de la vessie est bien connue. Il s’agit d’un repère fondamental en imagerie du pelvis.
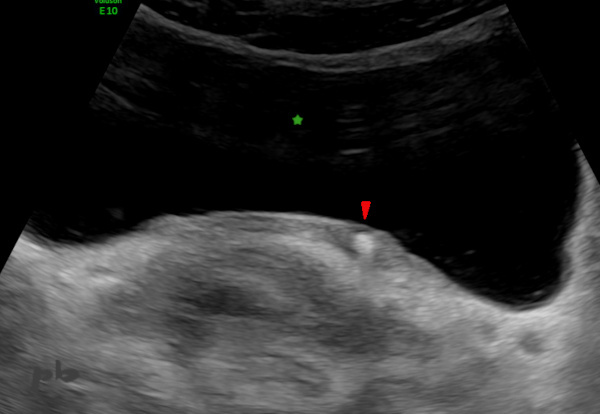
Attention cependant à ne pas prendre un volumineux kyste ovarien (★) pour une vessie pleine. Ceci peut arriver lorsque la vessie est vide (★), plaquée vers le bas et plus ou moins masqué par la symphyse pubienne.
1 – Pseudobladder
Abdominal ultrasound.
The ultrasound appearance of the bladder is well known. It is a fundamental landmark in pelvic imaging.
Be careful, however, not to mistake a large ovarian cyst (★) for a full bladder. This can happen when the bladder is empty (★), pressed downwards, and more or less obscured by the pubic symphysis.
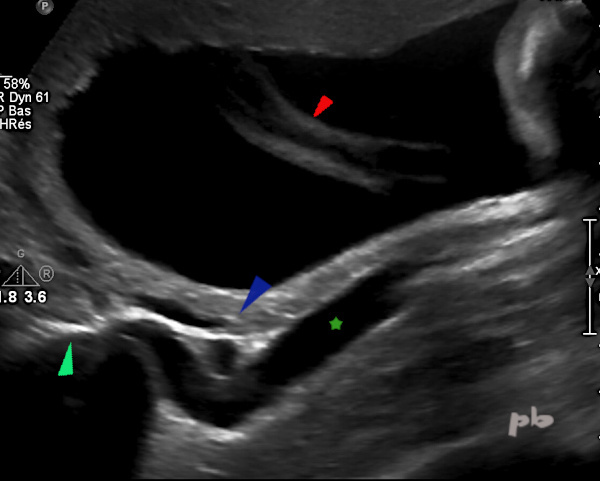
2 – Uretère normal – Péristaltisme
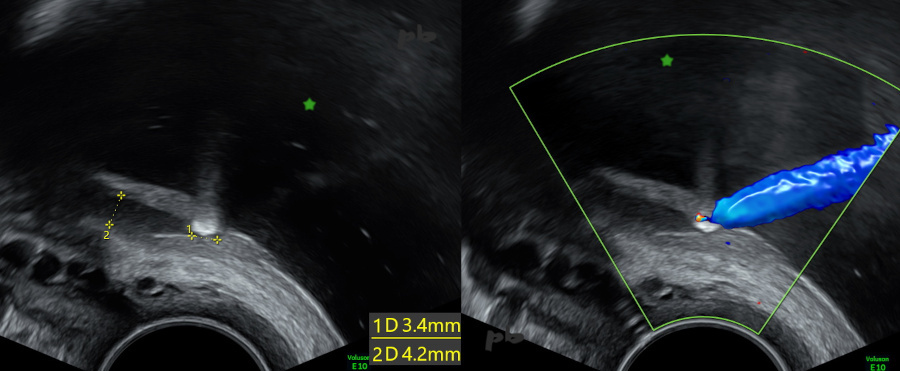
Visualisation lors d’une échographie par voie vaginale d’un segment de l’uretère pelvien lors du passage d’un flux d’urine (entre les croix). En aval, l’uretère est plat (►).
Aspect tout à fait physiologique, à ne pas confondre avec un hydrosalpinx par exemple.
2 – Normal ureter – Peristalsis
Visualization during a transvaginal ultrasound of a segment of the pelvic ureter during the passage of a urine flow (between the crosses). Downstream, the ureter is flat (►).
This is a completely physiological appearance and should not be confused with a hydrosalpinx, for example.
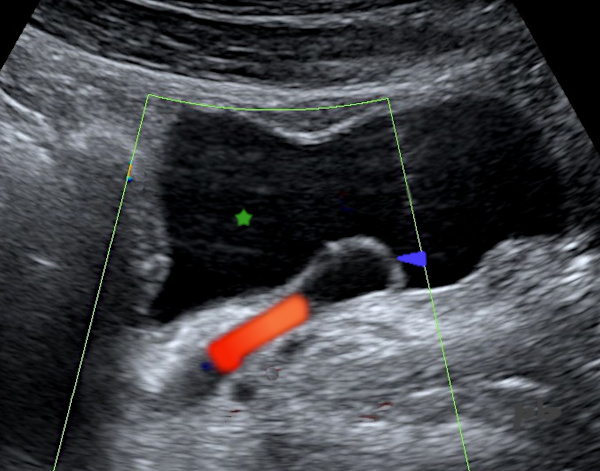
3 – Uretère normal – Péristaltisme
Vidéo.
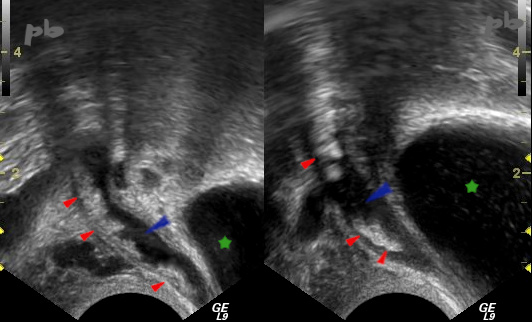
Visualisation lors d’une échographie par voie vaginale d’un segment de l’uretère pelvien lors du passage d’un flux d’urine. Il est suivi jusqu’à son abouchement dans la vessie (★)
Encore une fois, aspect tout à fait physiologique s’il redevient plat après le passage d’urines.
Utérus (♦)
3 – Normal Ureter – Peristalsis
Video.
Visualization during a transvaginal ultrasound of a segment of the pelvic ureter during the passage of a urine flow. It is followed until its opening into the bladder (★).
Once again, this is a completely physiological appearance if it becomes flat again after the urine passes.
Uterus (♦)
4 – Urétérocèle
Echographie par voie abdominale.
Coupe sagittale para-médiane.
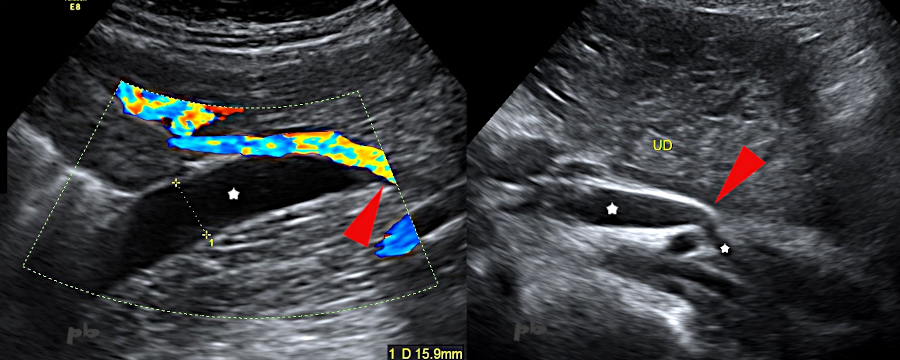
Dilatation de l’extrémité de l’uretère gauche (►), bombant dans la vessie (★).
En doppler couleur, le flux d’urine.
Une urétérocèle peut être de façon non rare associée à une duplication pyélo-urétérale.
4 – Ureterocele
Abdominal ultrasound. Parasagittal section.
Dilatation of the end of the left ureter (►), bulging into the bladder (★).
In color Doppler, the flow of urine.
A ureterocele can be associated with a pyelo-ureteral duplication.
5 – Urétérocèle
Echographie par voie vaginale. Vidéo.
Coupe sagittale para-médiane droite.
Urétérocèle droite (►) bombant dans la vessie (★).
L’uretère pelvien est modérément dilaté (étoile blanche).
Péristaltisme bien visible.
Elles sont le plus souvent de découverte fortuite et isolées, plus rarement retrouvées dans un contexte de malformation urinaire (ce qui était le cas ici).
5 – Ureterocele
Transvaginal ultrasound. Video.
Right paramedian sagittal section.
Right ureterocele (►) bulging into the bladder (★).
The pelvic ureter is moderately dilated (white star).
Peristalsis is clearly visible.
They are most often discovered incidentally and in isolation, more rarely found in the context of a urinary malformation (which was the case here).
6 – Lithiase
Echographie par voie abdominale vessie pleine (★). Coupe sagittale au niveau de l’abouchement urétéro-vésical.
Patiente présentant une douleur évocatrice de colique néphrétique à droite.
Dilatation du bas uretère pelvien (entre les croix 2), venant buter sur un calcul (croix 1).
6 – Lithiasis
Abdominal ultrasound with a full bladder (★). Sagittal section at the level of the ureterovesical junction.
Patient presenting with pain suggestive of right renal colic.
Dilatation of the lower pelvic ureter (between crosses 2), abutting on a stone (cross 1).
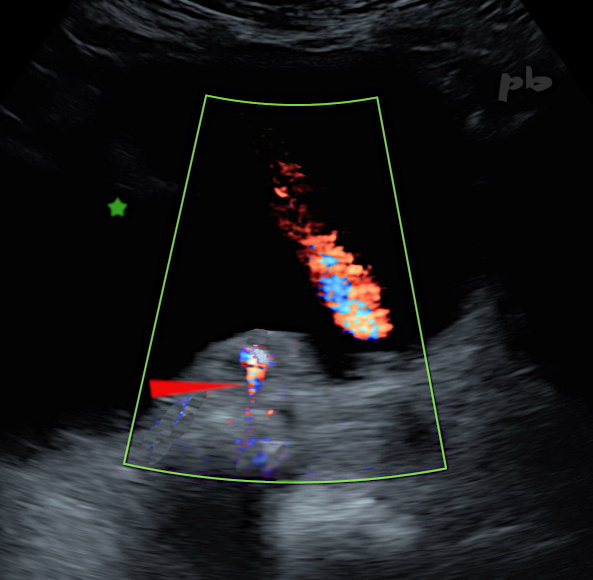
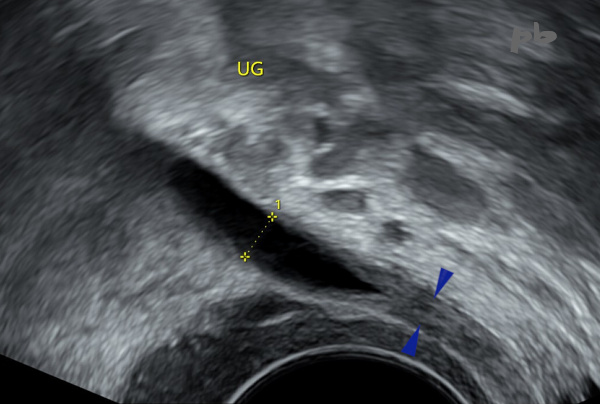
7 – Lithiase
(même patiente que 6)
Echographie par voie abdominale vessie pleine (★). Coupe transversale au niveau des abouchements urétéro-vésicaux, avec doppler couleur.
A droite, on retrouve le calcul hyperéchogène au niveau du méat. Artéfact de scintillement en arrière (►).
A gauche, beau jet urinaire.
7 – Lithiasis
(same patient as 6)
Abdominal ultrasound with a full bladder (★). Transverse section at the level of the ureterovesical junctions, with color Doppler.
On the right, there is a hyperechogenic stone at the level of the meatus. Twinkling artifact behind it (►).
Urinary jet on the left.
8 – Lithiase
Echographie par voie abdominale vessie semi-pleine (★). Coupe transversale au niveau des abouchements urétéro-vésicaux.
Patiente présentant une douleur évocatrice de colique néphrétique.
A gauche, zone hyperéchogène (►) sans cône d’ombre, compatible avec un calcul.
8 – Lithiasis
Abdominal ultrasound with a semi-full bladder (★). Transverse section at the level of the ureterovesical junctions.
Patient presenting with pain suggestive of renal colic.
On the left, a hyperechogenic area (►) without an acoustic shadow, compatible with a stone.
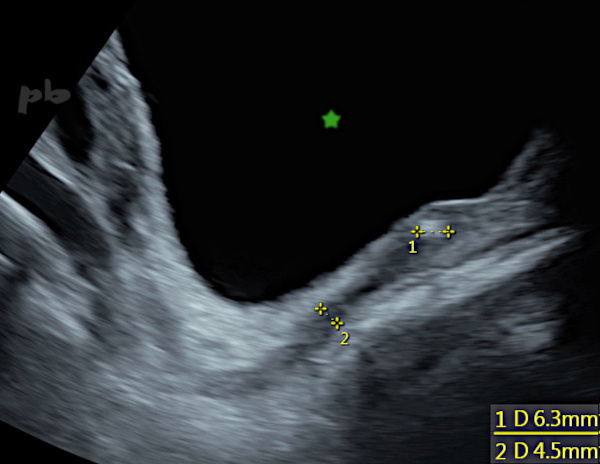
9 – Lithiase
(même patiente que 8)
Echographie par voie endovaginale.
Coupe sagittale au niveau de la jonction urétéro-vésicale gauche.
Dilatation du bas uretère pelvien (entre les croix 2), venant buter sur un calcul (croix 1) non calcifié (pas de cône d’ombre postérieur, artéfact de répétition). Présence d’un beau jet urinaire en doppler couleur sur l’image de droite, signant une obstruction incomplète.
Vessie (★)
9 – Lithiasis (same patient as 8)
Transvaginal ultrasound.
Sagittal section at the level of the left ureterovesical junction.
Dilatation of the lower pelvic ureter (between crosses 2), abutting on a non-calcified stone (cross 1) (no posterior shadow cone, repetition artifact). Presence of a good urinary jet in color Doppler on the right image, indicating incomplete obstruction.
Bladder (★)
10 – Lithiase – Grossesse
Coupe sagittale sur le bas uretère pelvien par voie vaginale.
Patiente enceinte à 38 SA.
Dilatation de l’uretère pelvien (►). Il est pavé de nombreux fragments lithiasiques (►) hyperéchogènes.
Vessie (★).
Si la voie sus-pubienne peut suffire (pas toujours) au diagnostic de calcul pelvien en-dehors de la grossesse, chez la femme enceinte, la voie vaginale devient vite indispensable – et très performante avec un peu d’habitude.
10 – Lithiasis – Pregnancy
Sagittal section of the lower pelvic ureter.Transvaginal ultrasound.
Patient pregnant at 38 weeks of gestation.
Dilatation of the pelvic ureter (►). It is lined with numerous hyper-echogenic lithiasic fragments (►).
Bladder (★)
While the abdominal echography may suffice (not always) for diagnosing pelvic stones outside of pregnancy, in pregnant women, the vaginal route quickly becomes essential—and very effective with a bit of practice.
11 – Urétéro-hydronéphrose et grossesse
Echographie abdominale. Coupes sagittales para-médianes sur l’uretère droit (étoile blanche) chez 2 patientes à 32 SA.
A gauche, l’uretère droit se termine « en queue de radis » au niveau du promontoire, en regard de la pince vasculaire constituée par les vaisseaux iliaques et ovariens (►). Cette dilatation est favorisée par la dextrorotation de l’utérus : aspect rencontré près d’une fois sur 2 pendant la grossesse, à considérer comme physiologique si la patiente est asymptomatique.
A droite au contraire, l’uretère droit se poursuit en intra-pelvien, témoignant d’un obstacle plus bas situé et non physiologique (voir images suivantes).
11 – Ureterohydronephrosis and Pregnancy
Abdominal Ultrasound. Sagittal paramedian sections of the right ureter (white star) in two patients at 32 weeks of gestation.
On the left, the right ureter ends in at the promontory level, because of the vascular clamp formed by the iliac and ovarian vessels (►). This dilation is favored by the dextrorotation of the uterus : an aspect encountered nearly one in two times during pregnancy, to be considered physiological if the patient is asymptomatic.
On the right, however, the right ureter continues into the pelvis, indicating a lower and non-physiological obstruction (see following images).
12 – Urétéro-hydronéphrose et grossesse
Echographie abdominale. Coupe sagittale oblique sur l’uretère droit (★) chez une patiente à 24 SA, présentant une douleur de type colique néphrétique.
Dilatation de l’uretère droit (★), passant en regard du promontoire (►), puis de la pince vasculaire (►). Pas de compression à ce niveau, la dilatation se poursuivant en-dessous. Il existait en fait un calcul au niveau du bas uretère.
Cordon ombilical (►) au sein du liquide amniotique
12 – Ureterohydronephrosis and Pregnancy
Abdominal Ultrasound. Oblique sagittal section of the right ureter (★) in a patient at 24 weeks of gestation, presenting with renal colic-like pain.
Dilatation of the right ureter (★), passing by the promontory (►), then the vascular clamp (►). No compression at this level, with the dilation continuing below. There was actually a stone in the lower ureter.
Umbilical cord (►) within the amniotic fluid.
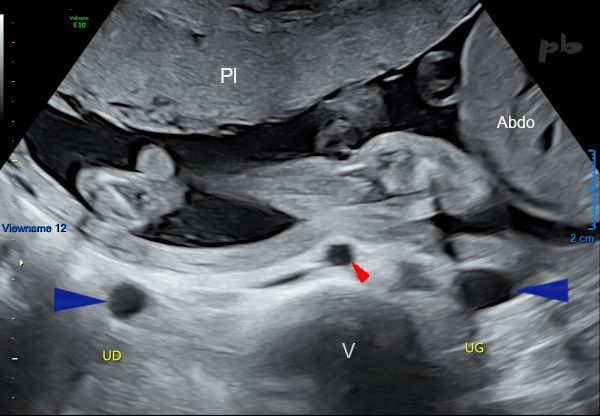
13 – Urétéro-hydronéphrose et grossesse
Echographie abdominale. Coupe transversale de l’abdomen maternel.
Patiente à 25 SA, présentant des douleurs lombaires bilatérales.
Dilatation des 2 uretères dans leur trajet lombaire (►). Cette dilatation ne dépassait pas le promontoire. Pas d’obstacle retrouvé en-dehors de l’utérus gravide.
Cette situation est fréquente à droite, mais très rare concernant le côté gauche : dans la majorité des cas il existe en effet une cause non gravide à la dilatation (calcul).
Abdo = abdomen fœtal
V = corps vertébral
Pl = placenta
► aorte maternelle
13 – Ureterohydronephrosis and Pregnancy
Abdominal Ultrasound. Transverse section of the maternal abdomen. Patient at 25 weeks of gestation, presenting with bilateral lumbar pain.
Dilatation of both ureters in their lumbar course (►). This dilation did not extend beyond the promontory. No obstruction found outside the gravid uterus.
This situation is common on the right side but very rare concerning the left side : in most cases, there is indeed a non-pregnancy-related cause for the dilation (stone).
Abdo = fetal abdomen
V = vertebral body
Pl = placenta
► maternal aorta
© Dr Philippe BASSNAGEL – 2025