
14 – Urétéro-hydronéphrose et hyperstimulation
Vidéo avec doppler couleur.
Uretère très dilaté (étoile blanche) en lombaire. Il s’arrête en regard du promontoire (►), au contact d’un volumineux ovaire hyperstimulé (★) : compression
En dessous, l’artère iliaque primitive se divisant en artère iliaque externe (AIE) et interne (AII). Encore en dessous, la veine iliaque.
14 – Uretero-hydronephrosis and hyperstimulation
Video with color Doppler.
Highly dilated ureter (white star) in the lumbar region. It stops at the level of the promontory (►), in contact with a large hyperstimulated ovary (★) : compression.
Below, the primitive iliac artery dividing into the external iliac artery (EIA) and internal iliac artery (IIA). Further below, the iliac vein.
15 – Sonde JJ
(même patiente que 12)
Echographie sus-pubienne.
Patiente à 24 SA, ayant présenté une colique néphrétique droite sur calcul.
Une sonde JJ a été posée, dont on voit parfaitement la boucle intra-vésicale (►).
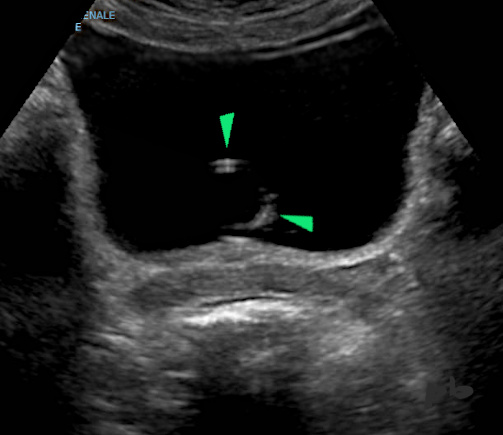
15 – JJ Stent (same patient as 12)
Suprapubic ultrasound.
Patient at 24 weeks gestation, who presented with right renal colic due to a stone.
A JJ stent was placed, and the intravesical loop (►) is clearly visible.
16 – Sonde JJ
Sonde JJ chez une patiente enceinte, posée après colique néphrétique sur calcul.
La boucle intra-vésicale (►) est englobée dans des concrétions calcaires (★).
Ce phénomène d’incrustation calcique est une complication non rare chez la femme enceinte.
Vessie (★)
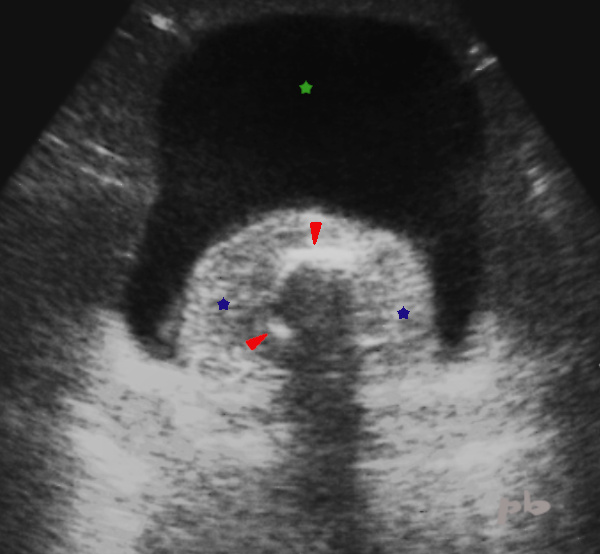
16 – JJ Stent
JJ stent in a pregnant patient, placed after renal colic due to a stone.
The intravesical loop (►) is encased in calcareous concretions (★).
This phenomenon of calcium encrustation is a not uncommon complication in pregnant women.
Bladder (★)
17 – Tumeur vésicale
Echographie endovaginale.
Coupe sagittale à gauche et frontale à droite. Le haut de la patiente est en haut sur l’image.
Petite masse tissulaire (►) d’échogénicité moyenne, de contours réguliers, d’allure bénigne, avec flux en doppler couleur.
En IRM, la tumeur était de même signal T2 que la paroi vésicale.
L’anapath a conclue à un léiomyome (bénin).
Vessie (★)
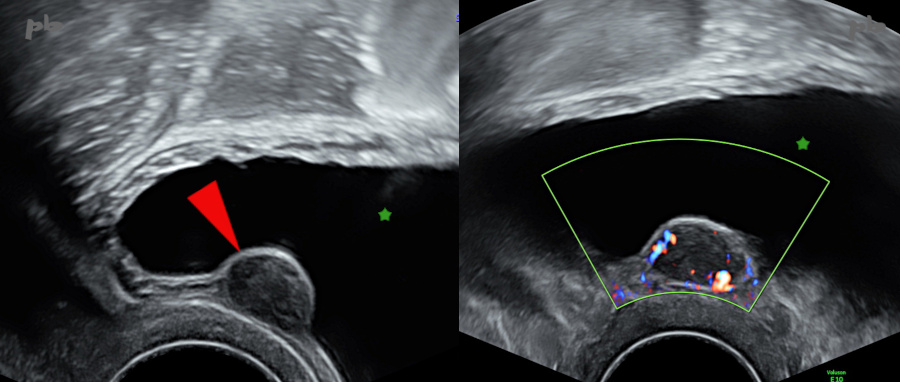
17 – Bladder Tumor
Transvaginal ultrasound. Sagittal section on the left and frontal section on the right. The top of the patient is at the top of the image.
Small tissue mass (►) of medium echogenicity, with regular contours, appearing benign, with flow on color Doppler.
On MRI, the tumor had the same T2 signal as the bladder wall. Pathology concluded it was a leiomyoma (benign).
Bladder (★)
18 – Rein pelvien
Echographie endovaginale
Reconnaitre un rein pelvien (►) lors d’une échographie pelvienne n’est pas toujours évident, surtout par voie vaginale.
Il faut y penser devant la découverte d’une masse tissulaire du petit bassin, de grande taille, chez une patiente par ailleurs asymptomatique.
Et regarder la fosse lombaire homolatérale…
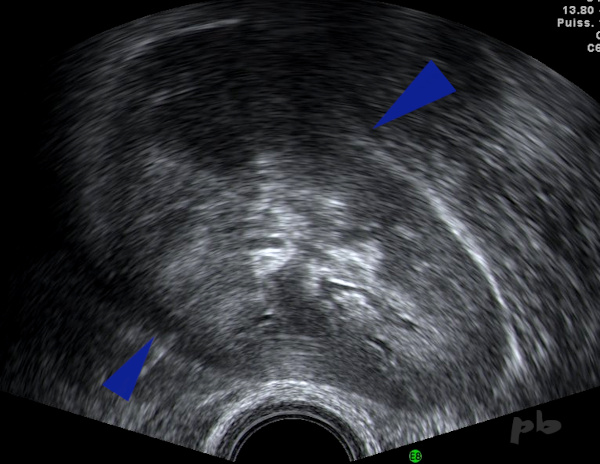
18 – Pelvic Kidney
Transvaginal ultrasound.
Recognizing a pelvic kidney (►) during a pelvic ultrasound is not always straightforward, especially via the vaginal route. It should be considered when discovering a large tissue mass in the pelvis in an otherwise asymptomatic patient.
And one should examine the homolateral lumbar fossa…
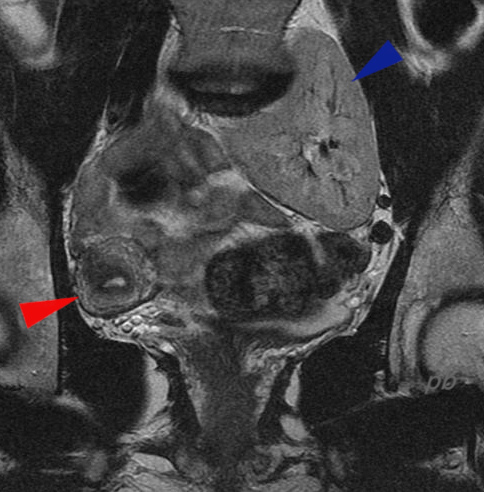
19 – Rein pelvien
(même patiente que 18)
IRM coupe frontale montrant le rein pelvien gauche (►).
On doit toujours penser à la possibilité d’une malformation utérine associée. L’IRM avait été réalisée pour confirmer l’existence d’un utérus unicorne droit (► U4b) vu à l’échographie (et non pour le rein pelvien).
19 – Pelvic Kidney
(same patient as 18)
MRI frontal section showing the left pelvic kidney (►).
One should always consider the possibility of an associated uterine malformation. The MRI was performed to confirm the presence of a right unicornuate uterus (► U4b) seen on ultrasound (and not for the pelvic kidney).
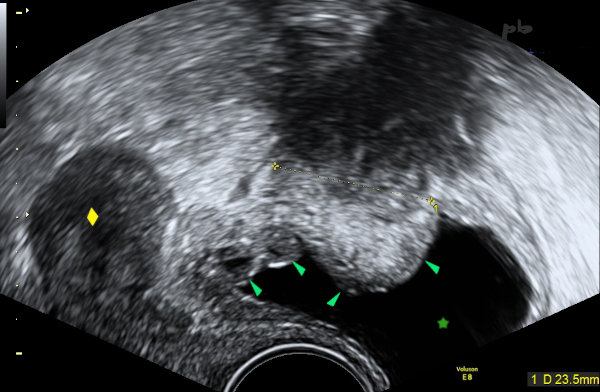
20 – Résidu de l’ouraque et surinfection – Faux positif d’endométriose
Echographie endo-vaginale coupe sagittale.
Douleurs pelviennes chez une patiente ménopausée. Traitement hormonal pendant plusieurs années et arrêtée récemment.
Présence d’une masse (entre les croix) située au-dessus de la vessie (★). Elle est globalement hypoéchogène et atténuante, et s’étend vers le haut, vers la paroi abdominale antérieure.
La paroi vésicale est infiltrée (►), irrégulière et déformée.
Utérus (♦)
20 – Urachal Remnant and Superinfection – False Positive for Endometriosis
Transvaginal ultrasound, sagittal section.
Pelvic pain in a menopausal patient. Hormonal treatment for several years and recently stopped.
Presence of a mass (between the crosses) located above the bladder (★). It is hypoechoic and attenuating, and extends upwards towards the anterior abdominal wall. The bladder wall is infiltrated (►), irregular, and deformed.
Uterus (♦)
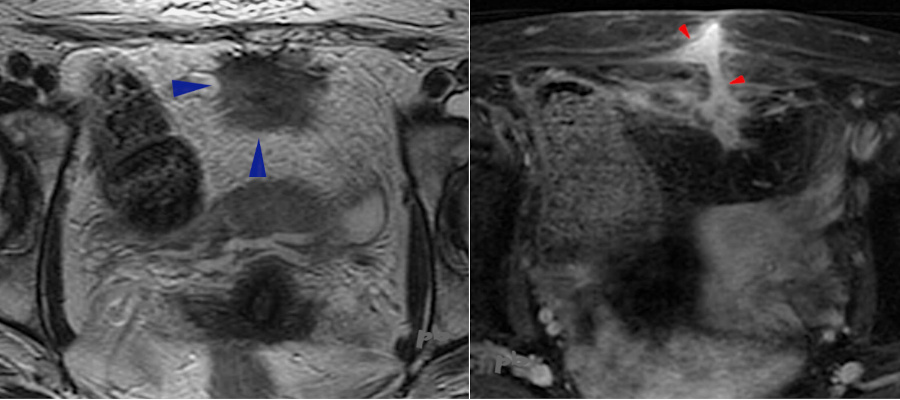
21 – Résidu de l’ouraque et surinfection – Faux positif d’endométriose
(même patiente que 20)
IRM réalisée 2 semaines plus tard. 2 coupes axiales, T2 à gauche et T1 avec gadolinium à droite.
Masse d’allure fibreuse (►), spiculée antérieure et médiane, sus-vésicale.
A droite, la coupe est plus haute, montrant une structure linéaire (►), prenant le contraste, et atteignant la face profonde musculaire antérieure.
-> Image étendue du dôme vésical à la paroi abdominale antérieure (au niveau d’une ancienne cicatrice), faisant évoquer une localisation endométriosique avec surinfection et fistule.
La fistule va s’ouvrir à la peau encore 15 jours plus tard, s’accompagnant de la régression des symptômes. La patiente sera finalement opérée, et l’anapath conclura à un trajet fistuleux implanté sur un résidu de canal ouraquien. Pas d’endométriose.
21 – Urachal Remnant and Superinfection – False Positive for Endometriosis (same patient as 20)
MRI performed 2 weeks later. Two axial sections, T2 on the left and T1 with gadolinium on the right.
An anterior mass with a fibrous appearance (►), spiculated, above the bladder.
On the right, the section is higher, showing a linear structure (►) that takes up contrast and reaches the deep anterior muscular surface.
-> An extensive image from the bladder dome to the anterior abdominal wall (at the level of an old scar), suggesting an endometriotic location with superinfection and fistula.
The fistula will open to the skin 15 days later, accompanied by the regression of symptoms. The patient will eventually undergo surgery, and pathology will conclude with a fistulous tract implanted on a remnant of the urachal canal. No endometriosis.
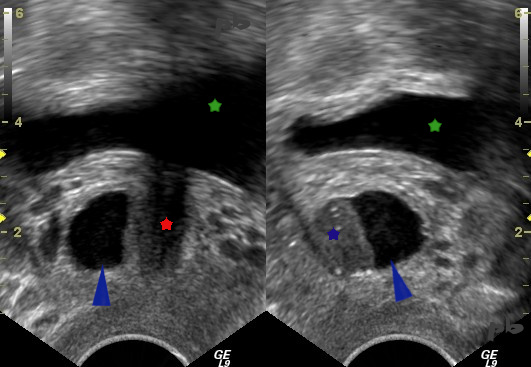
22 – Kyste para-urétral
Echographie endovaginale.
Coupe frontale à gauche et para-sagittale droite à droite. Le haut de la patiente est en haut sur l’image.
Le kyste (►) est liquidien avec un sédiment échogène (★). Il se situe à droite de l’urètre (★) sur la coupe frontale.
Vessie (★)
22 – Paraurethral Cyst
Transvaginal ultrasound. Frontal section on the left and parasagittal section on the right. The top of the patient is at the top of the image.
The cyst (►) is fluid-filled with an echogenic sediment (★). It is located to the right of the urethra (★) in the frontal section.
Bladder (★).

23 – Kyste para-urétral
Echographie endovaginale.
Coupe sagittale médiane. Le haut de la patiente est en haut sur l’image.
Autre exemple de kyste para-urétral (►) liquidien avec sédiment échogène (★). Il se situe en arrière de l’urètre (★).
Vessie (★)
Il s’agit le plus souvent de découverte fortuite, mais il est intéressant de les rechercher en cas d’infections urinaires à répétition.
23 – Paraurethral Cyst
Endovaginal ultrasound. Median sagittal section. The top of the patient is at the top of the image.
Another example of a fluid-filled paraurethral cyst (►) with echogenic sediment (★). It is located behind the urethra (★).
Bladder (★)
These are most often incidental findings, but it is interesting to look for them in cases of recurrent urinary tract infections.
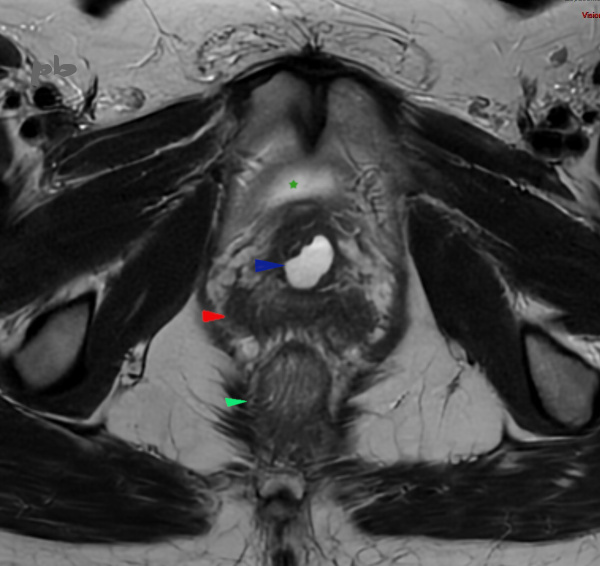
24 – Kyste para-urétral
IRM coupe axiale T2.
Autre exemple de kyste para-urétral (►) liquidien, en hypersignal T2.
Vessie (★)
Vagin (►)
Canal anal (►)
24 – Paraurethral Cyst – MRI T2 section
Another example of a fluid-filled paraurethral cyst (►). Hypersignal T2.
Bladder (★)
Vagina (►)
Anal canal (►)
© Dr Philippe BASSNAGEL – 2025