
1 – Hématométrie
Coupe sagittale par voie endovaginale.
Important épaississement central (►) hypoéchogène au myomètre et hétérogène. Contours nets et réguliers.
On voit la zone s’insinuer dans le canal cervical (★), en faveur d’une localisation endocavitaire.
Mouvements particulaires en temps réel. Pas de flux en doppler couleur (non montré)
Pas d’endomètre visible.
Volumineuse hématométrie (IVG la veille). Diagnostic différentiel d’un épaississement endométrial.
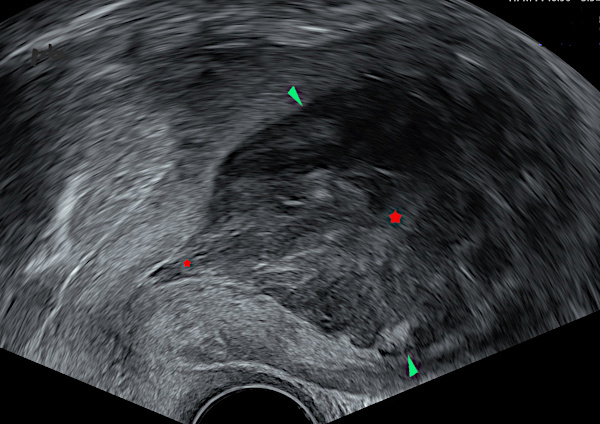
1 – Hematometra
Sagittal view via endovaginal ultrasound.
Significant central hypoechoic thickening (►) within the myometrium, with heterogeneous appearance. The borders are sharp and regular. The area is seen extending into the cervical canal (★), suggesting an intracavitary location. Particular movements observed in real-time. No color Doppler flow (not shown). No visible endometrium.
Large hematometra (medical abortion the previous day). Differential diagnosis of endometrial thickening.
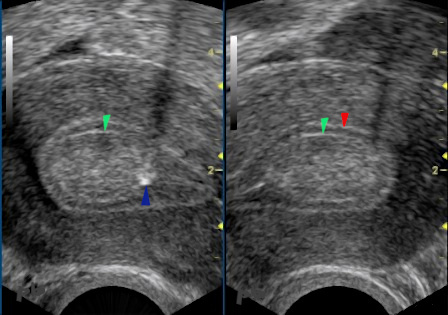
2 – Hypertrophie endométriale
Coupe sagittale par voie endovaginale.
*Endomètre très épaissi (22,5 mm entre les croix), sous stimulation par FSH, à J11.
*Echostructure homogène.
*Epaisseur régulière de chaque feuillet endométrial : un peu de liquide (►) permet de bien localiser la cavité.
*L’interface avec le myomètre est nette et régulière.
Simple hypertrophie endométriale.
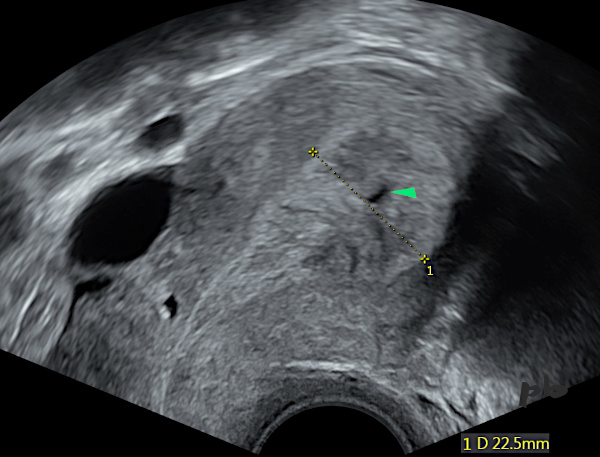
2 – Endometrial Hypertrophy
Sagittal view via endovaginal ultrasound.
Markedly thickened endometrium (22.5 mm between the crosses), under FSH stimulation, on day 11. Homogeneous echotexture. Regular thickness of each endometrial layer: a small amount of fluid (►) helps clearly locate the cavity. The interface with the myometrium is sharp and regular.
Simple endometrial hypertrophy.
3 – Hypertrophie endométriale
Coupes sagittales par voie endovaginale.
Métrorragies en période péri-ménopausique sous progestatif.
Image gauche :
* Endomètre épaissi (18,9 mm entre les croix).
* Echostructure homogène, avec rares images ovalaires hypoéchogènes (►) : glandes.
* la cavité n’est pas individualisée.
* L’interface avec le myomètre est nette et régulière.
Image droite : plusieurs flux vasculaires, répartis régulièrement.
Conclusion : épaississement sans signe suspect en imagerie.
Curetage : l’histologie retrouve un endomètre en atrophie glandulo-kystique.
Un endomètre épaissi en imagerie peut correspondre à une atrophie histologique. C’est un cas de figure classique avec le tamoxifène (voir plus loin).
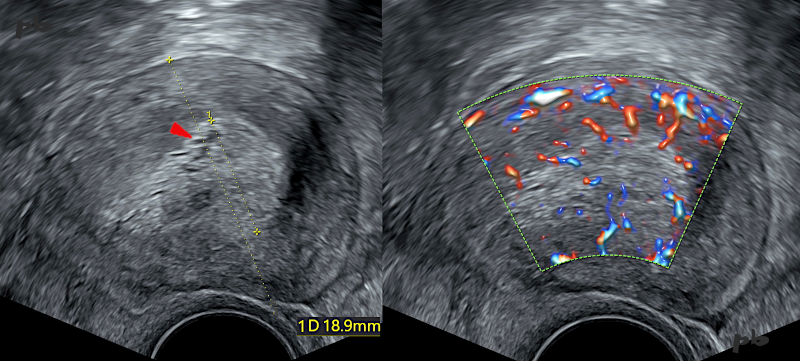
3 – Endometrial Hypertrophy
Sagittal view via endovaginal ultrasound. Metrorrhagia in the perimenopausal period under progestin therapy.
Left image:
* Thickened endometrium (18.9 mm between the crosses).
* Homogeneous echotexture, with rare hypoechoic oval images (►): glands.
* The cavity is not individualized.
* The interface with the myometrium is sharp and regular.
Right image: Multiple vascular flows, evenly distributed.
Conclusion: Thickening without suspicious imaging signs. Dilation and curettage performed. Histology reveals glandular-cystic atrophy of the endometrium. A thickened endometrium on imaging can correspond to histological atrophy. This is a classic scenario with tamoxifen (see further details later).
4 – Hypertrophie et glandes endométriales
Coupe sagittale par voie endovaginale. J45 du cycle.
– Endomètre épaissi.
– Echostructure homogène avec plusieurs petites images kystiques intra-endométriales (glandes ►).
– Epaisseur régulière de chaque feuillet endométrial : la ligne dite de vacuité, hyperéchogène (►), permet de bien localiser la cavité utérine.
-L’interface avec le myomètre est nette et régulière.
Simple hypertrophie avec glandes endométriales assez grosses pour devenir visibles en échographie du fait de la prolongation du cycle comme on le voit dans les grossesses débutantes.
Attention à ne pas confondre avec un sac gestationnel dans un contexte de suspicion de GEU (voir chapitre GEU image 9).
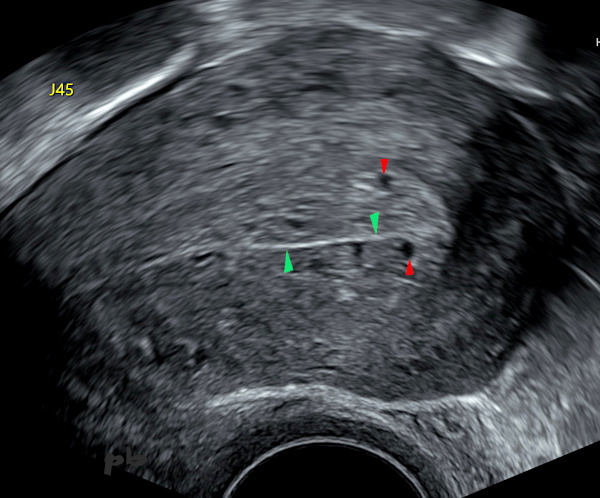
4 – Endometrial Hypertrophy and Glands
Sagittal section via endovaginal ultrasound. Day 45 of the cycle.
– Thickened endometrium.
– Homogeneous echotexture with several small intra-endometrial cystic images (glands ►).
– Regular thickness of each endometrial layer: the so-called « vacuity line, » which is hyperechoic (►), helps clearly locate the uterine cavity.
– The interface with the myometrium is sharp and regular.
This is a simple hypertrophy with endometrial glands large enough to be visible on ultrasound due to cycle prolongation, as seen in early pregnancy.
Caution: Do not confuse this with a gestational sac in cases of suspected ectopic pregnancy (see Ectopic Pregnancy chapter, image 9).

5 – Polype – Echographie
Coupe sagittale par voie endovaginale.
* les 2 feuillets endométriaux se séparent en regard d’une image hyperéchogène (★). L’ensemble donne un aspect de double contour. La mesure de l’endomètre doit se faire au niveau du losange ♦.
* Echostructure homogène de cette image avec un petit kyste interne (►).
* un peu de liquide (►) permet de bien localiser la cavité et moule la face inférieure du polype.
* L’interface avec le myomètre est nette et régulière.
* Ligne de vacuité (►).
Polype sans caractère suspect, responsable d’un pseudo- épaississement de l’endomètre.
5 – Polyp – Ultrasound
Sagittal section via endovaginal ultrasound.
* The two endometrial layers separate around a hyperechoic image (★), creating a double-contour appearance. Endometrial measurement should be taken at the diamond-shaped area (♦).
* Homogeneous echotexture of this image with a small internal cyst (►).
A small amount of fluid (►) helps clearly locate the cavity and outlines the lower surface of the polyp.
* The interface with the myometrium is sharp and regular.
* Vacuity line (►).
This is a polyp with no suspicious features, causing a pseudo-thickening of the endometrium.
6 – Polype
Echographie par voie endovaginale.
Aspect de double contour, avec le feuillet endométrial (►) d’une part, et la ligne de vacuité et le polype (►) d’autre part. La ligne de vacuité se présente sous la forme d’un trait hyperéchogène parfaitement net, en faveur de l’adossement de 2 structures anatomiques distinctes.
* Echostructure homogène du polype.
* Il refoule un DIU (►).
Polype sans caractère suspect, responsable d’un pseudo- épaississement de l’endomètre.
6 – Polyp – Endovaginal ultrasound.
Double-contour appearance, with the endometrial layer (►) on one side, and the vacuity line and the polyp (►) on the other. The vacuity line appears as a perfectly clear hyperechoic line, indicating the proximity of two distinct anatomical structures.
* Homogeneous echotexture of the polyp.
* It displaces an IUD (►).
This is a polyp with no suspicious features, causing a pseudo-thickening of the endometrium.
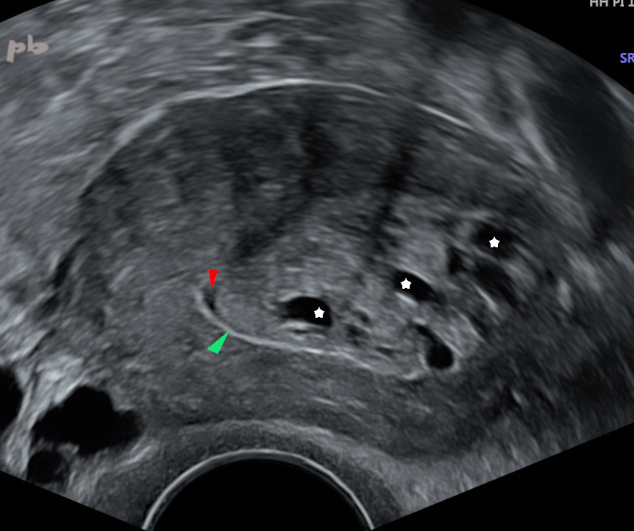
7 – Polype
Echographie par voie endovaginale.
Métrorragies chez une patiente ménopausée sans THS.
Volumineux épaissement endométrial hétérogène. Présence de plusieurs petits kystes internes (étoiles blanches).
On retrouve en inférieur sur l’image un trait net et hyperéchogène (►) en faveur d’une ligne de vacuité. Associée à l’existence d’un aspect de moulage par un peu de liquide (►), l’ensemble est en faveur d’une masse intra-cavitaire.
Volumineux polype glandulo-kystique. De façon générale, un endomètre épais et la présence de kystes multiples sont très évocateurs de la présence d’un polype.
7 – Polyp
Endovaginal ultrasound. Metrorrhagia in a postmenopausal patient without hormone replacement therapy (HRT).
Large, heterogeneous endometrial thickening. Presence of several small internal cysts (white stars). In the lower part of the image, there is a sharp, hyperechoic line (►), consistent with a vacuity line. Combined with the presence of molding by a small amount of fluid (►), this suggests an intracavitary mass.
Large glandular-cystic polyp. Generally, a thickened endometrium and the presence of multiple cysts are highly suggestive of a polyp.
8 – Polype
Echographie par voie endovaginale. Vidéo.
Volumineux épaissement endométrial homogène.
On distingue bien une image d’interface très nette (►), hyperéchogène, de type ligne de vacuité, en faveur de la présence d’une masse endo-cavitaire (★) et non d’un endomètre épais.
8 – Polyp
Endovaginal ultrasound. Video.
Large, homogeneous endometrial thickening. A very sharp, hyperechoic interface (►), resembling a vacuity line, is clearly visible, suggesting the presence of an intracavitary mass (★) rather than a thickened endometrium.

9 – Polype
(même patiente que 8)
Echographie par voie endovaginale. Coupes transversales avec doppler couleur.
Pédicule vasculaire (►). Il est très évocateur de polype, et fréquemment visualisé, mais pas toujours (en particulier chez les femmes ménopausées).
9 – Polyp
(Same patient as in image 8)
Endovaginal ultrasound. Transverse sections with color Doppler.
Vascular pedicle (►). This is highly suggestive of a polyp and is frequently visualized, though not always (particularly in postmenopausal women).
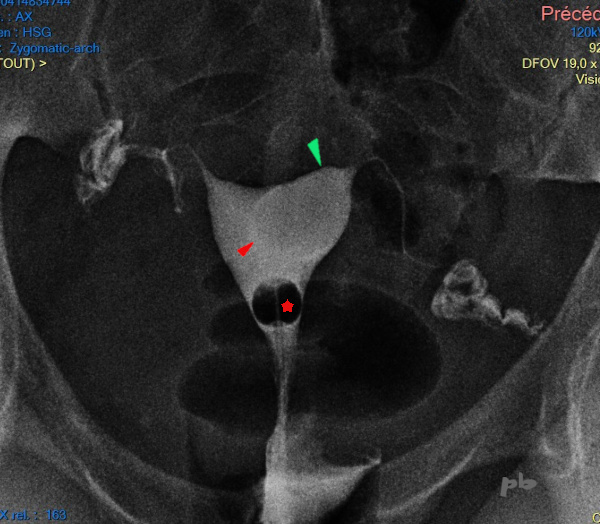
10 – Polype
Hystérographie (réalisée dans un contexte d’infertilité). Pour rappel cet examen n’est plus pratiqué pour la recherche et l’exploration des anomalies intra-cavitaires.
Image arrondie (►) moulée par le produit de contraste, à contours nets et réguliers. La corne utérine gauche (►) est distendue.
L’image ronde inférieure en négatif (★) correspond au ballonnet du cathéter d’injection.
10 – Polyp
Hysterosalpingography (performed in the context of infertility). This procedure is no longer used for the detection and exploration of intracavitary abnormalities.
Rounded image (►) outlined by the contrast medium, with sharp and regular contours. The left uterine horn (►) is distended.
The lower round negative image (★) corresponds to the balloon of the injection catheter.
© Dr Philippe BASSNAGEL – 2023