
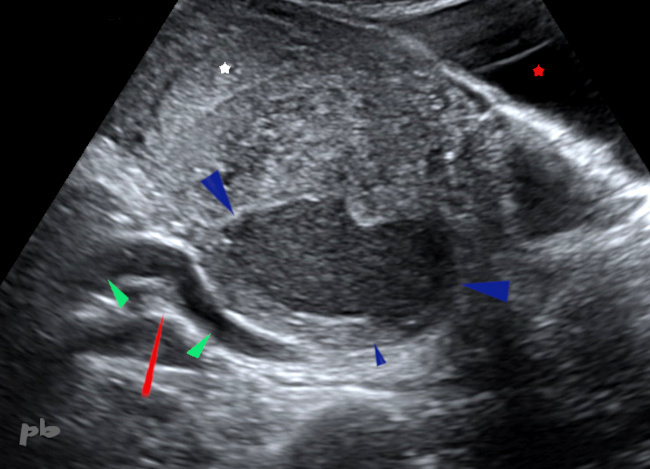
22- Kyste endométriosique – Echo
Balayage dans le plan sagittal.
Masse multikystique endométriosique (★) d’échogénicité moyenne, parsemée de fines images linéaires hyperéchogènes (►) et de amas plus grossiers : aspect échographique typique.
Il existe chez cette patiente une endométriose profonde associée.
Présence en périphérie du kyste de petites images liquidiennes (►) à ne pas confondre avec des follicules : pseudo-kystes péritonéaux.
On ne perçoit pas de délimitation très nette entre l’utérus et les ovaires qui forment ensemble un bloc adhérentiel.
Utérus (★).
Ovaire (★) contro-latéral avec plusieurs follicules.
22 – Endometriotic Cyst – Ultrasound
Sagittal plane scan.
A multicystic endometriotic mass (★) with intermediate echogenicity, interspersed with fine hyperechoic linear images (►) and coarser clusters : a typical ultrasonographic appearance. This patient also has associated deep endometriosis. Small fluid collections (►) are present at the periphery of the cyst and should not be confused with follicles : these are peritoneal pseudocysts. There is no clear demarcation between the uterus and the ovaries, which form an adhesive mass together.
Uterus (★).
Contralateral ovary (★) with multiple follicles.
23-Syndrome de Turner – Kyste endométriosique
IRM ax T1 fatsat
Image hypersignal T1 chez une patiente porteuse d’un syndrome de Turner.
De rares cas sont décrits dans la littérature, en cas de mosaïque XO/XX.
Un kyste endométriosique peut également être rencontré chez une patiente ménopausée.
23 – Turner Syndrome – Endometriotic Cyst Axial T1 fat-saturated MRI T1 hyperintense image in a patient with Turner syndrome. Few cases are described in the literature, particularly in XO/XX mosaicism. An endometriotic cyst may also be encountered in postmenopausal patients.
24 – Kyste endométriosique- Carcinome ovarien
Echo et doppler couleur
Kyste endométriosique ovarien droit à contenu hypoéchogène, finement particulaire (★). Présence de quelques images végétantes endokystiques non vascularisées (►).
Localisations d’endométriose profonde par ailleurs (non montrées).
24 – Endometriotic Cyst – Ovarian Carcinoma Ultrasound and Color Doppler
Right ovarian endometriotic cyst with hypoechoic, finely particulate content (★). Presence of a few non-vascularized endocystic vegetations (►). Deep endometriosis lesions are also present elsewhere (not shown).
25 – Kyste endométriosique-Carcinome ovarien
(Même patiente que 24)
IRM axial T1 fatsat.
Kyste endométriosique sur chaque ovaire (★) en hypersignal T1, contenant de petites images végétantes (►). Pas de prise de contraste après injection.
La patiente est opérée peu après : endométriose stade 4. Kystectomie ovarienne droite.
Kyste endométriosique confirmé en anapath.
25 – Endometriotic cyst – Ovarian carcinoma (Same patient as 24)
Axial T1-weighted MRI with fat saturation Endometriotic cysts on each ovary (★) showing high T1 signal, containing small vegetating images (►). No contrast enhancement after injection.
The patient underwent surgery shortly afterward : stage 4 endometriosis. Right ovarian cystectomy. Endometriotic cyst confirmed by histopathological examination.
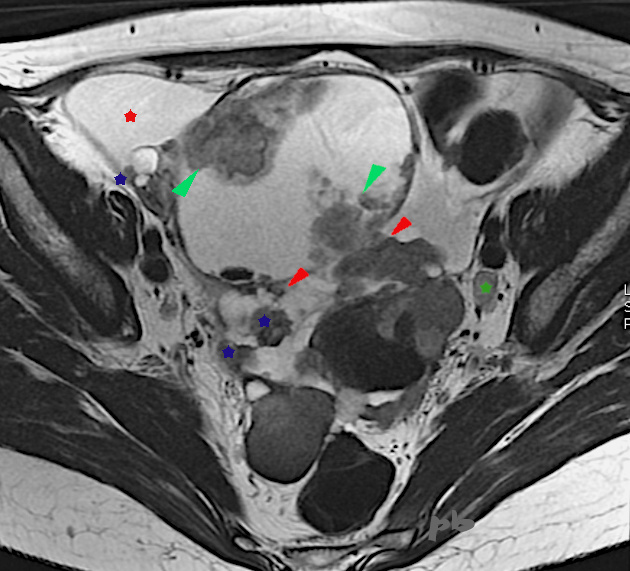
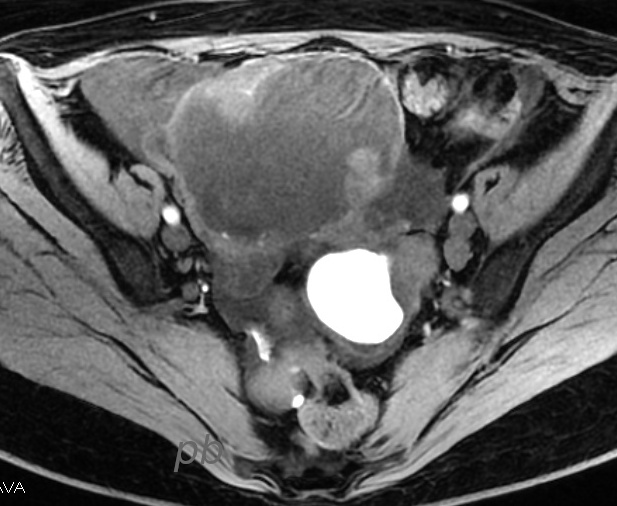
26 – Kyste endométriosique-Carcinome ovarien
(Même patiente que 24)
IRM axial T2
10 mois plus tard, récidive du kyste droit.
Volumineux kyste à droite, contenant des végétations internes (►) et externes (►).
Les zones tissulaires s’étendent sur le péritoine (★). On en retrouve en particulier en sus-vésical et dans le Douglas (non montrées).
Ascite (★).
Adénopathie iliaque gauche (★)
Prise de contraste après injection de gado.
Conclusion : Tumeur ovarienne maligne et carcinomatose péritonéale.
26 – Endometriotic cyst-Ovarian carcinoma (Same patient as in case 24)
Axial T2 MRI .
10 months later, recurrence of the right cyst. Large cyst on the right, containing internal (►) and external (►) vegetations. Tissue areas extend to the peritoneum (★), particularly in the suprapubic region and the Douglas pouch (not shown).
Ascites (★). Left iliac lymphadenopathy (★)
Contrast enhancement after gadolinium injection.
Conclusion : Malignant ovarian tumor and peritoneal carcinomatosis.
27 – Kyste endométriosique-Carcinome ovarien
(Même patiente que 24)
IRM axial T1
On retrouve la composante hémorragique du kyste ovarien gauche, en hypersignal T1, avec des végétations plus exubérantes.
Une biopsie péritonéale a pu être réalisée, confirmant l’adénocarcinome très probablement d’origine ovarienne.
Ce dossier permet de rappeler le lien qui existe entre endométriose et certains types de cancers ovariens, endométrioïdes en particulier.
27 – Endometriotic cyst-Ovarian carcinoma
(Same patient as in case 24)
Axial T1 MRI
The hemorrhagic component of the left ovarian cyst is visible, showing high T1 signal, with more exuberant vegetations.
A peritoneal biopsy was performed, confirming adenocarcinoma most likely of ovarian origin.
This case highlights the link between endometriosis and certain types of ovarian cancers, particularly endometrioid carcinomas.
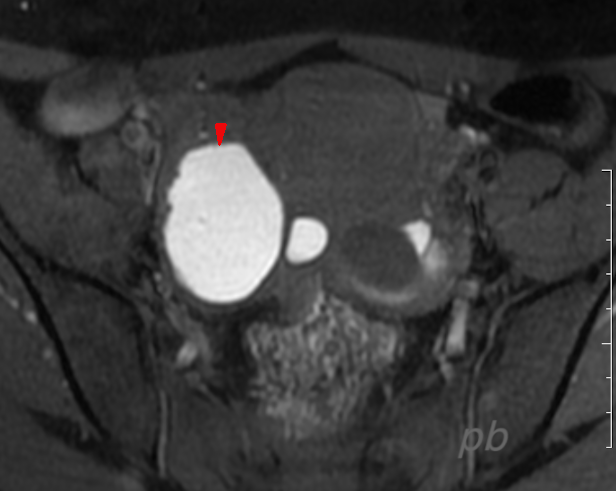
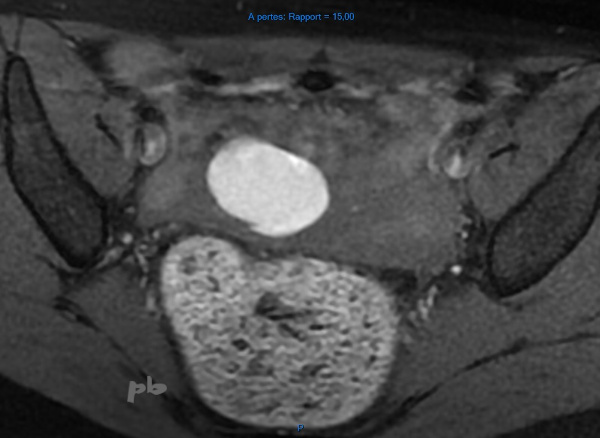
28-Endométriome – IRM
Coupe axiale T1 fatsat.
Endométriome typique en hypersignal T1 (►).
28 – Endometrioma – MRI
Axial T1 fat-saturated image.
Typical endometrioma with high T1 signal (►).

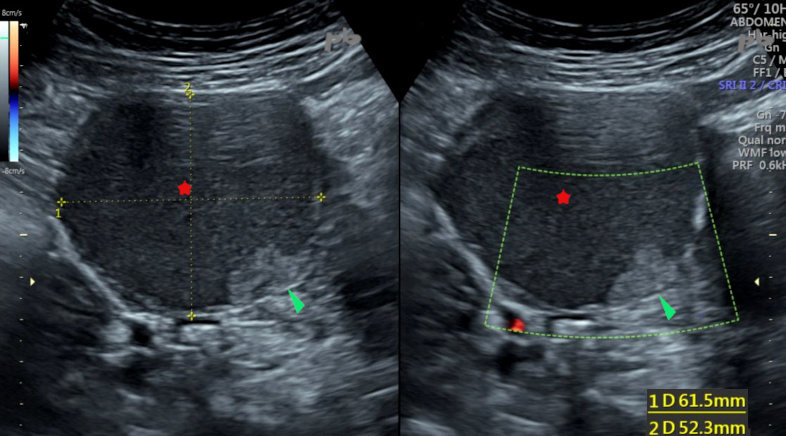
29- Endométriome – Echo-doppler
(Même patiente que 28)
Examen réalisé quelques mois plus tard : patiente enceinte, à 28 SA.
Aspect atypique du kyste endométriosique connu (►), qui contient une plage centrale hyperéchogène, vascularisée.
29 – Endometrioma – Doppler ultrasound
(Same patient as in case 28)
Examination performed a few months later : pregnant patient, at 28 weeks of gestation.
Atypical appearance of the known endometriotic cyst (►), which contains a central hyperechoic, vascularized area.
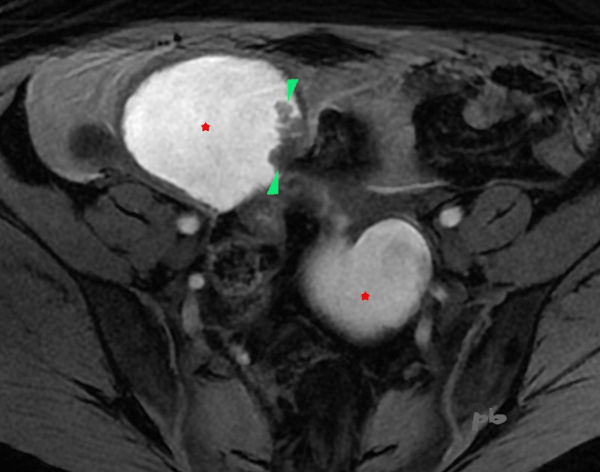
30- Endométriome – IRM
(Même patiente que 28)
Coupe axiale T1.
Examen réalisé peu après l’échographie : patiente à 30 SA.
Nette modification de l’aspect du kyste endométriosique ovarien droit (►) en IRM, dont une partie est en hyposignal T1.
Utérus gravide (★).
La patiente sera opérée à 8 mois post-partum : kyste endométriosique confirmé en anapath.
Les modifications du kyste pendant la grossesse correspondent vraisemblablement à des phénomènes de décidualisation. Ils sont particulièrement trompeurs.
30 – Endometrioma – MRI
(Same patient as in case 28) – Axial T1 image.
Examination performed shortly after the ultrasound : patient at 30 weeks of gestation. Marked change in the appearance of the right ovarian endometriotic cyst (►) on MRI, with part of it showing low T1 signal.
Gravid uterus (★).
The patient underwent surgery 8 months postpartum : the endometriotic cyst was confirmed on pathology.
The changes in the cyst during pregnancy likely correspond to decidualization phenomena. They are particularly misleading.
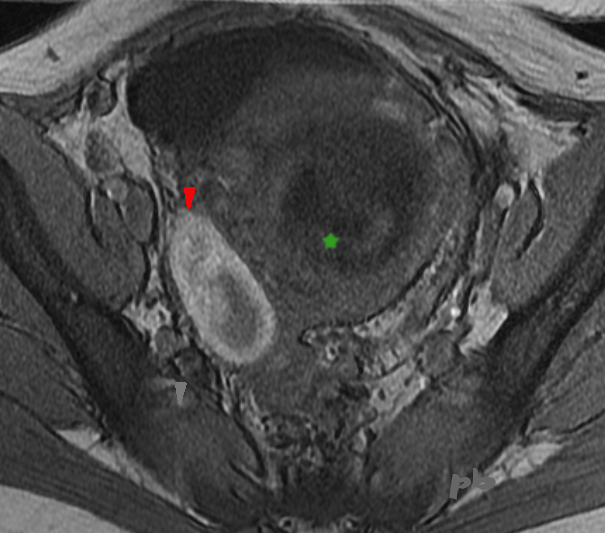
31 – Endométriome- Compression urinaire
Echographie par voie sus-pubienne. Coupe sagittale médiane.
Kyste endométriosique ovarien droit (►) comprimant l’uretère droit (►). La compression se situe en pelvien haut, un peu en-dessous du promontoire (►). L’uretère est visible au-dessus du promontoire, puis dans la concavité sacrée.
Hydronéphrose droite associée (non montrée).
L’utérus est en avant, paraissant collé au kyste (pas d’interface visible entre eux).
Contexte d’endométriose sévère avec localisation sur le torus et volumineux endométriome gauche.
Endomètre (étoile blanche)
Vessie (★)
31 – Endometrioma – Ureteral compression
Suprapubic ultrasound. Midline sagittal view.
Right ovarian endometriotic cyst (►) compressing the right ureter (►). The compression is located in the upper pelvis, just below the promontory (►). The ureter is visible above the promontory and then in the sacral concavity.
Associated right hydronephrosis (not shown).
The uterus is anterior, appearing adhered to the cyst (no visible interface between them).
Context of severe endometriosis with involvement of the torus and a large left endometrioma.
Endometrium (white star)
Bladder (★)
© Dr Philippe BASSNAGEL – 2021