
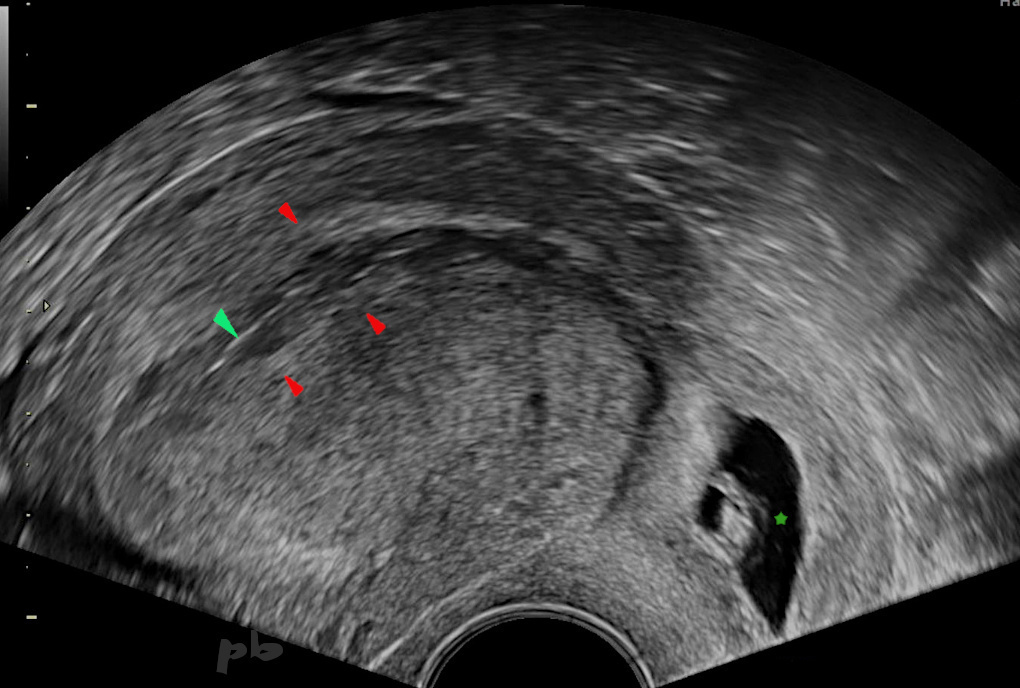
30- Grossesse ectopique cervicale
- Utérus rétrofléchi. Coupe sagittale.
- Endomètre (►) et ligne de vacuité ( ► ) hyperéchogène. Pas d’hématométrie.
- Le sac gestationnel est visualisé au niveau cervical (★); pas d’antécédent de césarienne.
- Il contenait un embryon vivant de 8 mm.
30- Cervical ectopic pregnancy
Retroflexed uterus. Sagittal section.
Hyperechogenic endometrium (►) and vacuity line (►). No hematometra.
The gestational sac is visualized at the cervical level (★) ; no history of cesarean section.
It contained a living embryo of 8 mm.
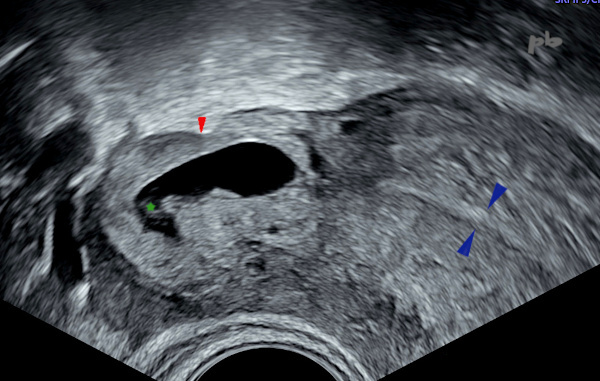
31- GEU – Grossesse ectopique isthmique
- Coupe sagittale par voie sus-pubienne.
- Sac gestationnel en situation isthmique (★).
- Fond de la cavité utérine (► ).
- La vessie est vide.
31- Isthmic Ectopic Pregnancy
Abdominal ultrasonography. Sagittal section.
Gestational sac in isthmic position (★).
Fundus of the uterine cavity (►).
The bladder is empty.
32- GEU – Grossesse ectopique isthmique (même patiente que 31)
- Par voie vaginale, le sac gestationnel est localisé en situation isthmique, au niveau d’une cicatrice d’hystérotomie (►).
- Lumière cervicale (► ).
- L’embryon était vivant.
32- Isthmic Ectopic Pregnancy (same patient as 31)
Transvaginal ultrasonography.
The gestational sac is located in the isthmic region, at the site of a hysterotomy scar (►).
Cervical lumen (►).
The embryo was alive.
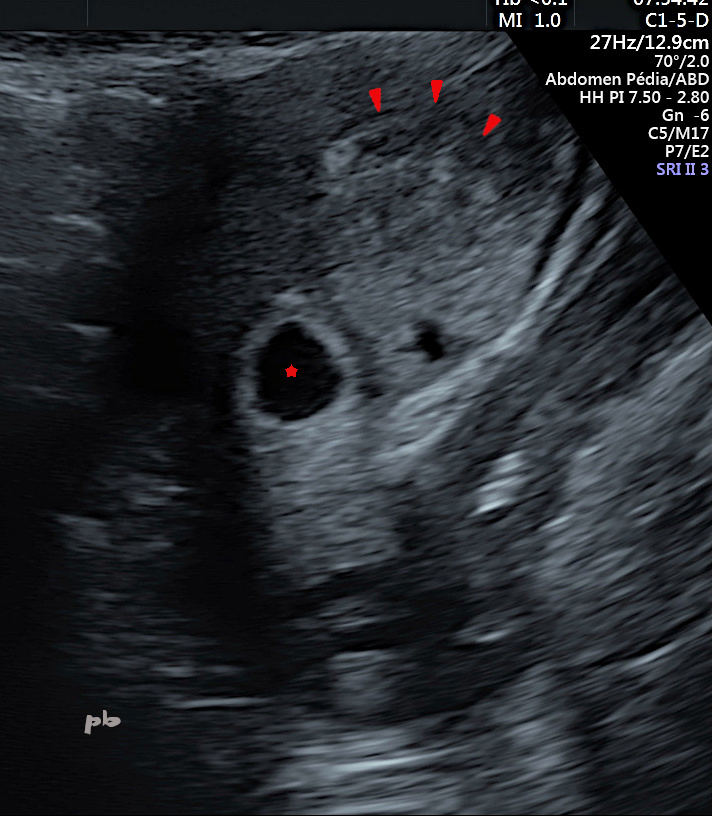
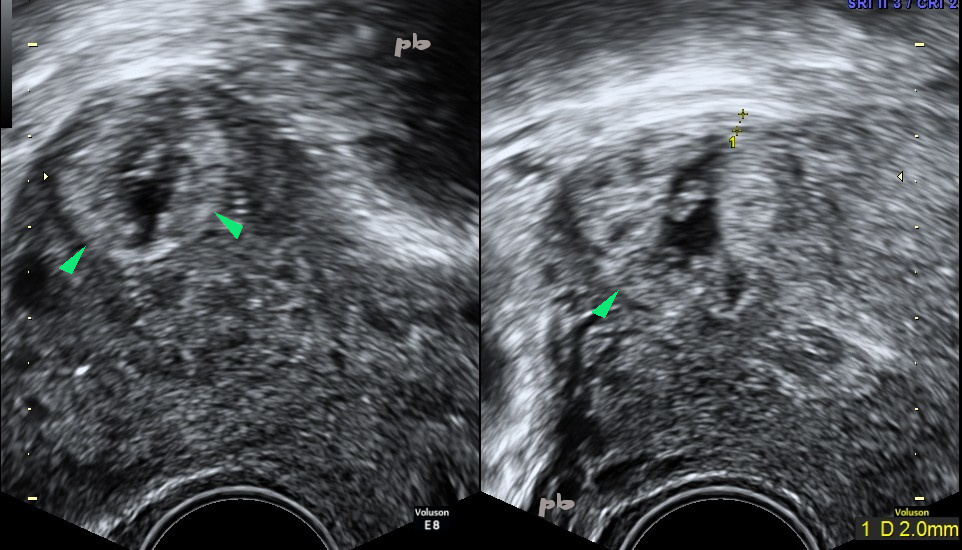
33- GEU interstitielle
Voie endo-vaginale.
Grossesse obtenue après stimulation ovarienne et réimplantation embryonnaire, située dans le segment interstitiel (ou intra-mural) de la trompe droite.
Pas de myomètre visualisé entre le bord utérin et le trophoblaste (►).
Sur l’image, on visualise le sac gestationnel en-dehors de la cavité.
Endomètre (►)
Embryon (★)
33- Interstitial Ectopic Pregnancy
Transvaginal ultrasonography.
Pregnancy achieved after ovarian stimulation and embryo reimplantation. The pregnancy is located in the interstitial (or intramural) segment of the right tube.
No myometrium visualized between the uterine edge and the trophoblast (►).
In the image, the gestational sac is visualized outside the cavity.
Endometrium (►)
Embryo (★)
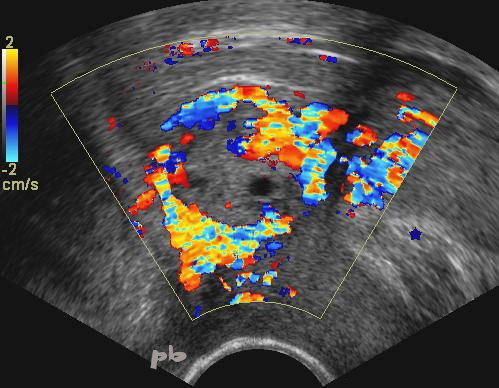
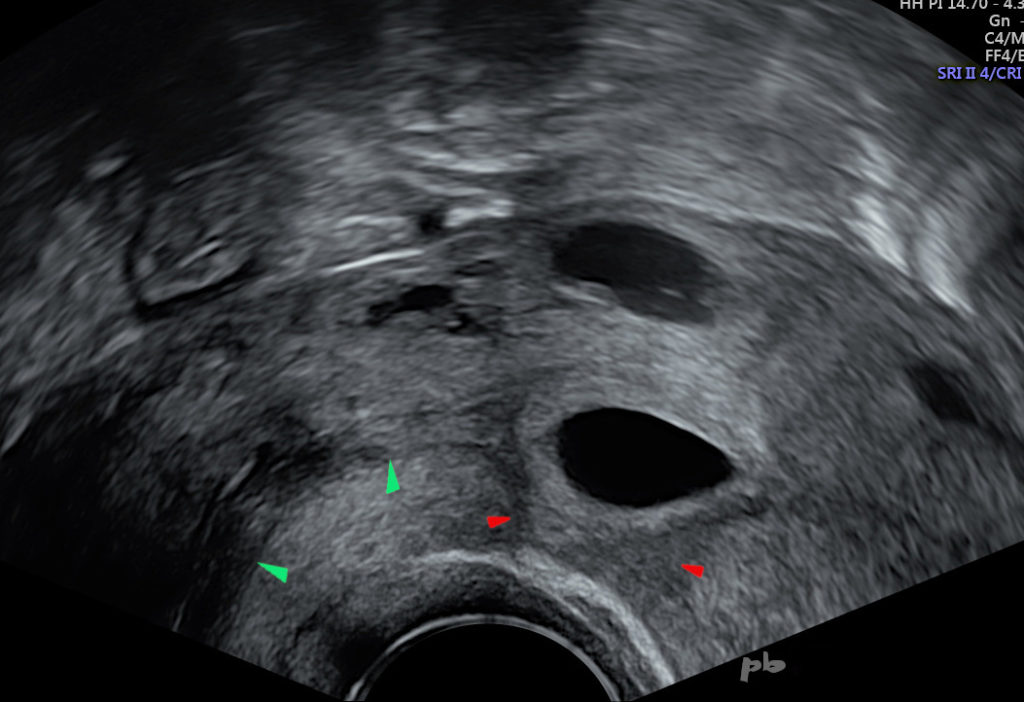
34- GEU interstitielle
- Voie endo-vaginale.
- Grossesse située dans le segment interstitiel de la trompe droite.
- Riche couronne vasculaire venant au contact de la séreuse utérine.
- L’endomètre (★) et la cavité sont bien visibles.
34- Interstitial Ectopic Pregnancy
Transvaginal ultrasonography.
Pregnancy located in the interstitial segment of the right tube.
Rich vascular crown coming into contact with the uterine serosa.
The endometrium (★) and the cavity are clearly visible.
35- GEU interstitielle
- Sac gestationnel (►) contenant un embryon.
- Il est très excentré, an niveau de la corne utérine, avec persistance d’une bande de myomètre en périphérie de 2 mm.
- Le diagnostic différentiel peut être difficile avec un sac excentré, dans la corne utérine, mais restant endo-cavitaire.
35 – Interstitial pregnancy
Gestational sac (►) containing an embryo.
It is highly eccentric, at the level of the uterine horn, with persistence of a 2 mm band of myometrium at the periphery (between the crosses).
The differential diagnosis can be difficult with an eccentric sac, in the uterine horn, but remaining endocavitary.

36- GEU interstitielle
(même patiente que 35)
- Agrandissement permettant de mieux distinguer l’embryon (★). Pas d’activité cardiaque.
- Vascularisation périphérique.
- Contours utérins (►).
36 – Interstitial pregnancy (same patient as 35)
Enlargement allowing better distinction of the embryo (★ ). No cardiac activity.
Peripheral vascularization.
Uterine contours ( ►).
37- GEU interstitielle
- Voie sus-pubienne.
- Volumineuse image « en cible » au niveau de la corne utérine gauche.
- Stagnation des B HCG. Curetage réalisé pour sac présumé intra-cavitaire : échec.
En fait le sac est situé en-dehors de la cavité et de l’endomètre (★). - On doit aussi penser à un diagnostic différentiel : le fibrome en nécrobiose, d’où l’IRM réalisée le lendemain.
37 – Interstitial ectopic pregnancy
Abdominal ultrasonography.
Large ‘target-like’ image at the level of the left uterine horn. Stagnation of beta hCG levels. Curettage performed for presumed intra-cavitary sac : failure.
In fact, the sac is located outside the cavity and the endometrium (★).
We must also consider a differential diagnosis : necrobiosis fibroid, hence the MRI performed the next day.
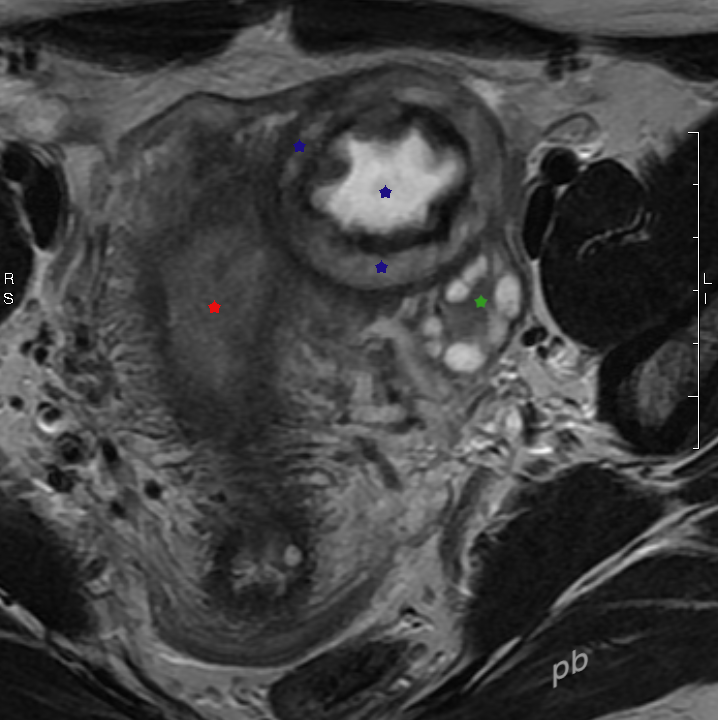
38- GEU interstitielle
(même patiente que 37)
- IRM réalisée le lendemain de l’échographie.
- Coupe transversale du pelvis en pondération T2. Coupe frontale de l’utérus.
- L’anatomie est beaucoup plus claire et plus globale.
- Volumineuse image « en cible » (★) au niveau de la corne utérine gauche.
- Ovaire gauche en arrière (★). Couronne folliculaire.
- Endomètre et cavité utérine (★). Zone jonctionnelle en périphérie, en hyposignal.
38 – Interstitial ectopic pregnancy (same patient as 37)
MRI performed the day after the ultrasound.
Transverse section of the pelvis in T2 weighting. Frontal section of the uterus.
The anatomy is much clearer and more comprehensive.
Large ‘target-like’ image (★) at the level of the left uterine horn. Ring in clear T2 hyposignal, hemorrhagic.
Left ovary behind (★). Follicular crown.
Endometrium and uterine cavity (★). Junctional zone on the periphery, in hyposignal.
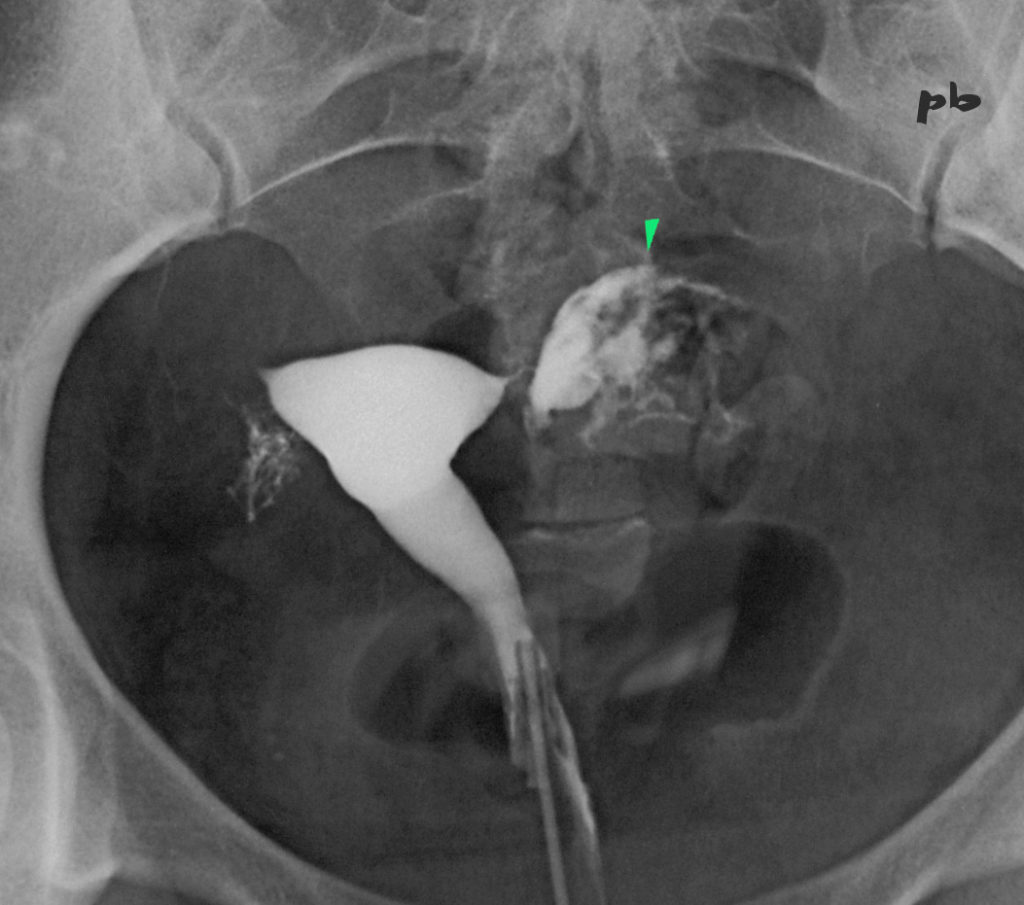
39- GEU interstitielle
(même patiente que 37)
- Hystérosalpingographie réalisée 2 mois plus tard.
β HCG à 0. - Opacification partielle d’une cavité intra-tubaire et myométriale (►).
39 – Interstitial ectopic pregnancy (same patient as 37)
Hysterosalpingography performed 2 months later.
Beta hCG at 0.
Partial opacification of an intra-tubal and myometrial cavity (►).
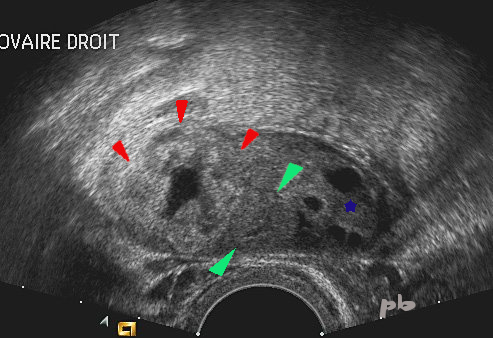
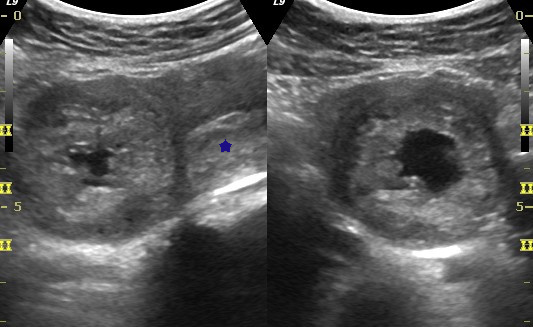
40-GEU ovarienne
Ovaire droit par voie vaginale :
- Tissu ovarien avec follicules (★)
- Corps jaune (►)
- GEU (►) : image « en cible ».
40 – Ovarian ectopic pregnancy
Right ovary via vaginal approach :
– Ovarian tissue with follicles (★)
– Corpus luteum (►)
– Ectopic pregnancy (►) : ‘target-like’ image.

41- GEU ovarienne
- Image « en cible » de 36 mm sur l’ovaire droit.
- Tissu ovarien au contact (★).
- La mobilisation avec la sonde vaginale de l’ovaire et de la masse aide à mieux localiser la grossesse, dans la trompe ou dans l’ovaire.
41 – Ovarian ectopic pregnancy
‘Target-like’ image of 36 mm on the right ovary.
Ovarian tissue in contact (★).
Mobilizing the ovary and the mass with the vaginal probe helps to better locate the pregnancy, whether in the tube or in the ovary.
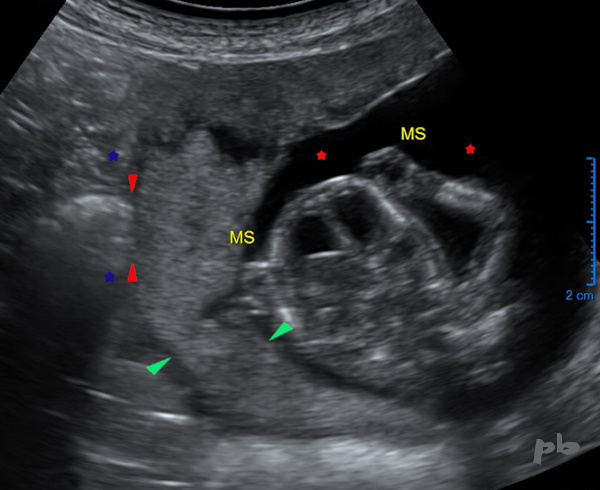
42 – Grossesse abdominale
1ère échographie à 13 SA.
Pas d’anomalie visualisée.
-MS = membres supérieurs. La tête au milieu.
-Liquide amniotique (![]() )
)
-Placenta (![]() )
)
Le tube digestif maternel (![]() ) est directement au contact de l’œuf, sans interposition de tissu utérin (
) est directement au contact de l’œuf, sans interposition de tissu utérin (![]() ).
).
Le diagnostic de grossesse abdominale ne sera porté finalement qu’un mois plus tard.
La localisation extra-utérine aurait été plus facilement retrouvée sur une échographie précoce.
42 – Abdominal pregnancy
First ultrasound at 13 weeks of gestation. No visible abnormalities.
MS = upper limbs. The head is in the middle.
Amniotic fluid (★)
Placenta (►)
The maternal digestive tract (★) is directly in contact with the egg, without interposition of uterine tissue (►).
The diagnosis of abdominal pregnancy will finally be made only a month later. The extrauterine location could have been more easily found on an early ultrasound.
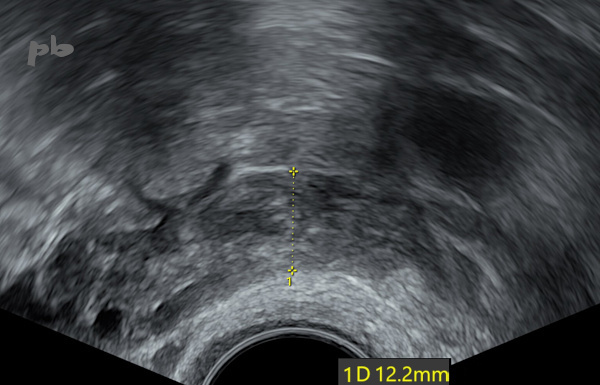
43 – GEU et salpingostomie
GEU gauche (sac gestationnel intra-tubaire) traitée par salpingostomie, à J4 post-chirurgie.
Baisse des B HCG, mais persistance des douleurs.
Echographie endovaginale.
La trompe (entre les croix) reste épaissie, hétérogène, mais de calibre régulier : simples caillots.
Normalisation clinique et échographique rapide.
43 – Ectopic pregnancy and salpingostomy
Left ectopic pregnancy (intra-tubal gestational sac) treated by salpingostomy on day 4 post-surgery.
Decrease in β-HCG levels, but persistence of pain.
Transvaginal ultrasound.
The tube (between the crosses) remains thickened, heterogeneous, but with a regular caliber: simple clots. Rapid clinical and ultrasonographic normalization.
© Dr Philippe BASSNAGEL – 2021