

35 – Utérus unicorne avec cavité non communicante
(U4a selon la classification de l’ESHRE)
IRM coupe axiale T2. Relecture.
Faux diagnostic de masse latéro-utérine droite de type kyste endométriosique.
Le centre de la masse était en hypersignal T1, hématique.
La corne utérine gauche est bien visualisée (►), mais non la droite. La masse apparait en fait d’origine utérine avec une cavité (hématique ★), une zone jonctionnelle (►) en hyposignal, et une couronne périphérique d’allure myométriale (★).
Il s’agit donc d’un utérus unicorne gauche avec hémi corps droit borgne.
Par ailleurs, follicule dominant à droite (►), nettement à distance, ce qui exclue d’autant plus l’origine ovarienne de la masse.
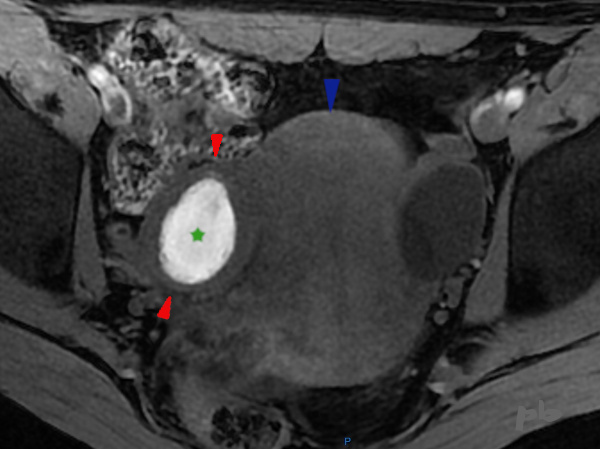
35 – Unicornuate uterus with non-communicating cavity (ESHRE classification U4a)
T2-weighted MRI, axial view. Re-review.
Misdiagnosis of a right latero-uterine mass initially thought to be an endometriotic cyst. The center of the mass showed T1 hyperintensity, consistent with blood content. The left uterine horn is clearly visualized (►), but the right horn is not. The mass appears to be of uterine origin, featuring:
– A cavity (hematic ★),
– A junctional zone (►) in hypointensity,
– A peripheral rim resembling myometrium (★).
This is therefore a left unicornuate uterus with a blind right hemi-body.
Additionally, a dominant follicle is visible on the right (►), clearly distant from the mass, further excluding an ovarian origin.

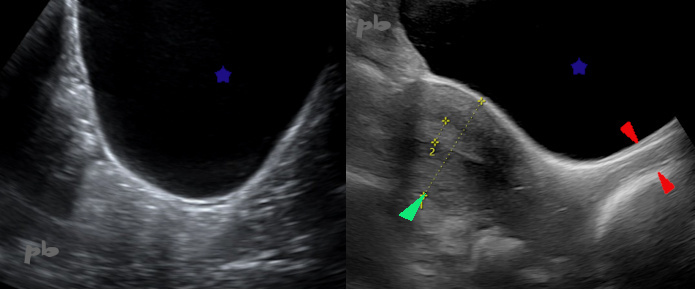
36 – Utérus unicorne avec cavité non communicante
(U4a selon la classification de l’ESHRE)
(même patiente que 35)
Echographie endovaginale effectuée un mois plus tard.
Les 2 hémi cavités sont bien visibles (★), hyperéchogènes. Aspect épaissi et contours irréguliers à droite en faveur d’un saignement chronique, et perte de la ligne de vacuité.
36 – Unicornuate uterus with a non-communicating cavity (U4a according to the ESHRE classification)
(Same patient as image 35)
A transvaginal ultrasound was performed one month later. Both hemi-cavities are clearly visible (★) and hyperechoic. The right side shows a thickened appearance with irregular contours, suggestive of chronic bleeding, and loss of the vacuity line.
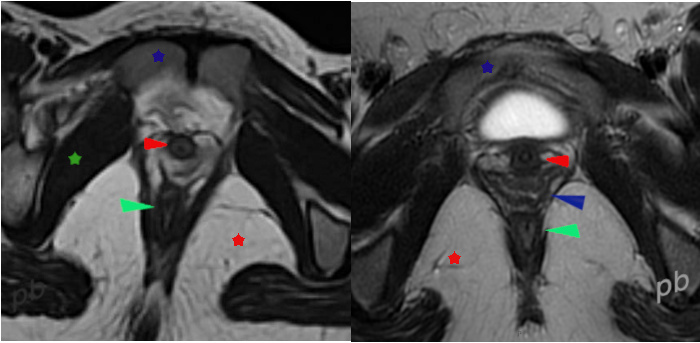
37 – Syndrome de Rokitanski-Kuster-Hauser
(U5b C4 V4 selon la classification de l’ESHRE)
Echographie par voie sus-pubienne.
Patiente âgée de 18 ans. Aménorrhée primaire.
Echo et IRM déjà réalisées, non contributives, mais pas d’examen clinique.
Dans un 2ème temps, elle consulte un gynécologue, qui l’examine, et l’adresse pour une nouvelle échographie.
Image gauche coupe sagittale : aucune structure utéro-vaginale n’est visualisée en arrière de la vessie (★). Le pelvis est entièrement occupé par des images digestives.
Image droite montrant l’aspect normalement attendu.
Vagin (►) Utérus (►).
37 – Mayer-Rokitansky-Küster-Hauser (MRKH) Syndrome (U5b C4 V4 according to the ESHRE classification)
Suprapubic ultrasound.
An 18-year-old patient with primary amenorrhea. Previous ultrasound and MRI were performed but were non-contributory; however, no clinical examination was conducted. Subsequently, she consults a gynecologist, who examines her and refers her for a new ultrasound. Left image (sagittal view): No uterovaginal structure is visualized behind the bladder (★). The pelvis is entirely occupied by digestive structures.
Right image: Shows the normally expected appearance.
Vagina (►), Uterus (►).
38 – Syndrome de Rokitanski-Kuster-Hauser
(même patiente que 37)
IRM coupe axiale T2 sur le plancher pelvien. Relecture.
Image gauche : aucune structure vaginale n’est visualisée entre l’urètre (►) et le canal anal (►).
Image droite montrant l’aspect normalement attendu.
Vagin (►). Pubis (★).
Muscle obturateur interne et canal d’Alcock (★).
Fosse ischio-rectale (★).
38 – Mayer-Rokitansky-Küster-Hauser (MRKH) Syndrome
(Same patient as image 37)
Axial T2 MRI of the pelvic floor. Review.
Left image: No vaginal structure is visualized between the urethra (►) and the anal canal (►).
Right image: Shows the normally expected appearance.
Vagina (►). Pubis (★). Obturator internus muscle and Alcock’s canal (★). Ischio-rectal fossa (★).
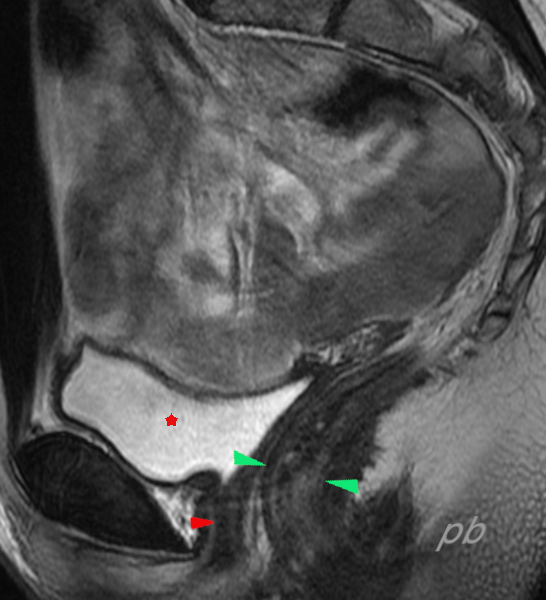
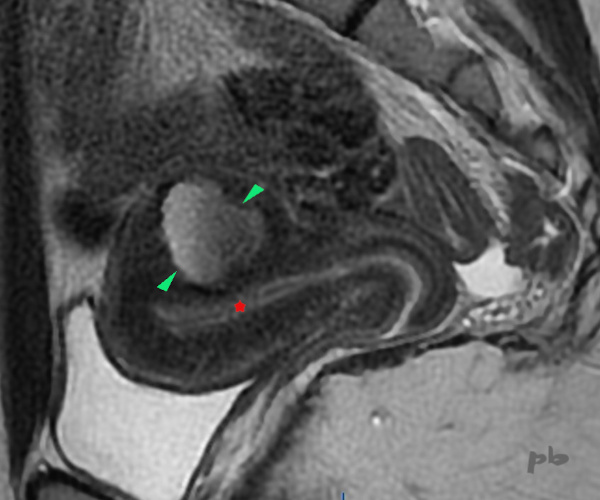
39 – Syndrome de Rokitanski-Kuster-Hauser
(U5b C4 V4 selon la classification de l’ESHRE)
IRM coupe sagittale T2 de l’ensemble du pelvis.
Pas d’utérus ni de vagin identifié.
Vessie (★).
Urètre (►).
canal anal (►).
39 – Mayer-Rokitansky-Küster-Hauser (MRKH) Syndrome (U5b C4 V4 according to the ESHRE classification)
Sagittal T2 MRI of the entire pelvis. No uterus or vagina is identified.
Bladder (★).
Urethra (►).
Anal canal (►).
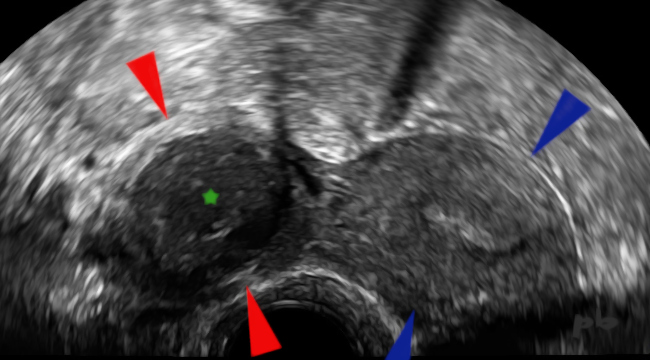
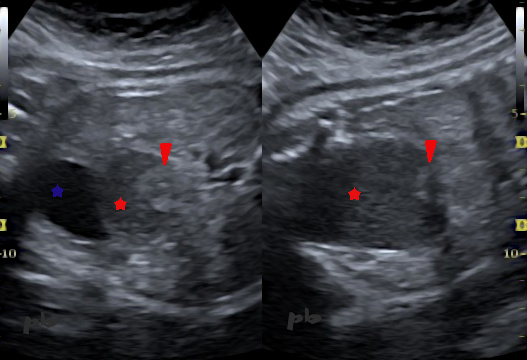
40 – Masse utérine cavitaire accessoire (MUCA)
Echographie endo-vaginale.
Douleurs pelviennes plus ou moins cycliques chez une jeune fille de 13 ans.
Coupe transversale sur l’utérus (►).
En latéro-utérin droit, présence d’une image arrondie (►) à paroi régulière, épaisse, et à contenu d’allure hématique (★).
L’ovaire droit était à distance et l’utérus de morphologie normale (2 cornes utérines).
40 – Accessory Cavitary Uterine Mass (ACUM)
Transvaginal ultrasound.
More or less cyclic pelvic pain in a 13-year-old girl. Transverse section of the uterus (►). On the right lateral side of the uterus, presence of a rounded image (►) with a regular, thick wall, and content appearing hematic (★). The right ovary was located at a distance, and the uterus had a normal morphology (2 uterine horns).

41 – Masse utérine cavitaire accessoire (MUCA)
(même patiente que 40)
IRM coupe axiale T2.
Coupe frontale sur l’utérus (►).
En latéro-utérin droit, on retrouve l’image arrondie (►) à paroi régulière, épaisse, et à contenu en hyposignal T2 (★).
L’ovaire droit était à distance.
A noter un kyste fonctionnel banal sur l’ovaire gauche (★).
41 – Accessory Cavitary Uterine Mass (ACUM)
(same patient as case 40)
MRI axial T2-weighted section. Coronal section of the uterus (►). On the right lateral side of the uterus, the rounded image (►) with a regular, thick wall and T2-hypointense content (★) is again observed. The right ovary was located at a distance. Note the presence of a simple functional cyst on the left ovary (★).
42 – Masse utérine cavitaire accessoire (MUCA)
(même patiente que 40)
IRM, coupe axiale T1.
Coupe frontale sur l’utérus (►).
En latéro-utérin droit, on retrouve l’image arrondie (►) dont le contenu est en hypersignal T1 (★), hématique.
L’anapath a confirmé le diagnostic de MUCA.
On aurait pu évoquer une hémi cavité utérine borgne sur un utérus bicorne, mais les 2 cornes utérines étaient parfaitement visibles et normales, en échographie comme en IRM (non montré).
Pour plus de détails : European Radiology (2019) 29:1144-1152
42 – Accessory Cavitary Uterine Mass (ACUM)
(same patient as case 40)
MRI axial T1-weighted image. Frontal section of the uterus (►). In the right lateral uterine region, a rounded image (►) is visible, with T1 hyperintense content (★), consistent with blood. Pathology confirmed the diagnosis of ACUM. A blind hemicavity in a bicornuate uterus could have been considered, but both uterine horns were clearly visible and normal on both ultrasound and MRI (not shown).
For further details: European Radiology (2019) 29:1144-1152
43 – Masse utérine cavitaire accessoire (MUCA)
IRM – Coupe sagittale T2.
Utérus antéversé, dont la paroi postérieure présente une image arrondie en plein myomètre, (►) en hypersignal T2 modéré.
Exérèse per-coelioscopique confirmant le diagnostic.
La localisation intra-utérine a aussi été décrite dans ces anomalies embryologiques.
Endomètre (★).
43 – Accessory Cavitary Uterine Mass (ACUM)
MRI – Sagittal T2-weighted image.
An anteverted uterus, with the posterior wall showing a rounded image within the myometrium (►), moderately hyperintense on T2. Laparoscopic excision confirmed the diagnosis. Intrauterine location has also been described in these embryological anomalies.
Endometrium (★).
44 – Imperforation hyménéale de découverte anténatale
(V3 selon la classification de l’ESHRE)
Echographie réalisée à 34 SA.
Coupe transversale à gauche et frontale du fœtus à droite.
Image discrètement hypoéchogène (★) de topographie abdomino-pelvienne, chez un fœtus de sexe féminin.
Elle se situe juste en arrière de la vessie (★).
Petite image hyperéchogène interne (►).
44 – Prenatally Diagnosed Hymen Imperforation (V3 according to the ESHRE classification)
Ultrasound performed at 34 weeks of gestation. Transverse section on the left and frontal section of the fetus on the right.
A slightly hypoechoic image (★) in the abdominopelvic region in a female fetus. It is located just posterior to the bladder (★). Small internal hyperechoic image (►).
45 – Imperforation hyménéale de découverte anténatale
(V3 selon la classification de l’ESHRE)
(même patiente que 44)
IRM réalisée le même jour.
Coupe frontale du fœtus en pondération T2.
Image de signal intermédiaire (★) de topographie abdomino-pelvienne.
Elle s’étend depuis le périnée jusqu’au niveau abdominal.
Petite image supérieure en hyposignal (►) correspondant à l’image vue en écho : col utérin bombant dans un volumineux hématocolpos.
Confirmation à la naissance. Pas d’autres anomalies, en particulier de cloaque.
Vésicule biliaire (★).
Poumons (★).
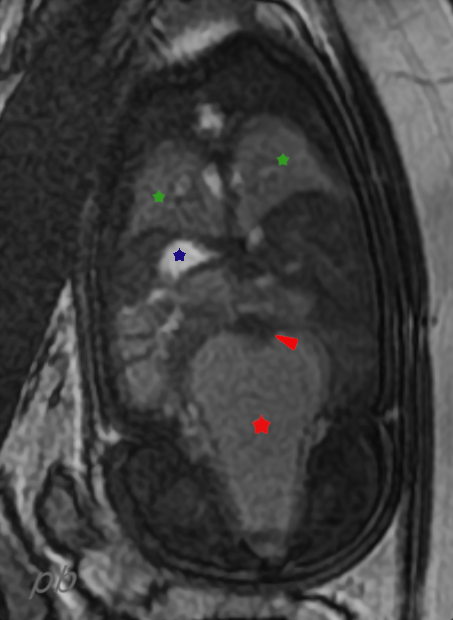
45 – Prenatally Diagnosed Hymen Imperforation (V3 according to the ESHRE classification)
(same patient as 44)
MRI performed on the same day. Frontal T2-weighted image of the fetus. An intermediate signal image (★) in the abdominopelvic region. It extends from the perineum to the abdominal level. Small superior hypointense image (►) corresponding to the ultrasound finding: a bulging uterine cervix within a large hematocolpos.
Gallbladder (★). Lungs (★).
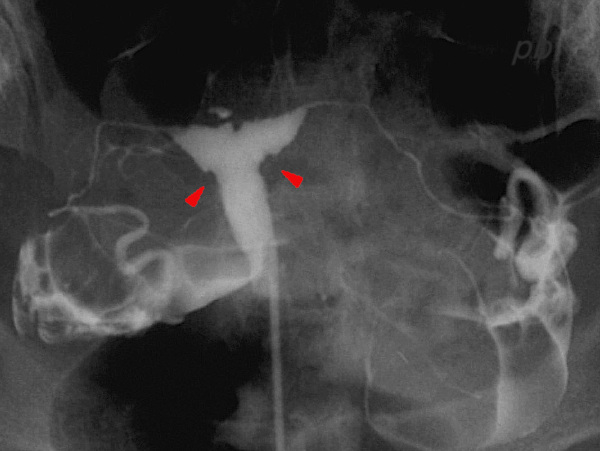
46 – Utérus Distilbène (DES)
(U1a selon la classification de l’ESHRE)
Hystérographie (HSG)
Contours cavitaires irréguliers, en particulier à l’origine des 2 cornes (►), donnant cet aspect de morphologie en « T », évocateur de l’utérus DES.
46 – DES-related Uterus (Diethylstilbestrol) (ESHRE classification: U1a)
Hysterosalpingography (HSG): Irregular uterine cavity contours, particularly at the origin of the two horns (►), resulting in a « T-shaped » morphology, suggestive of a DES-related uterus.
© Dr Philippe BASSNAGEL – 2022